Division of Pediatric Hematology, Oncology, and Blood and Marrow Transplantation, Department of Pediatrics, and.
Division of Biostatistics, Medical College of Wisconsin, Milwaukee, WI.
Blood. 2019 Feb 14;133(7):754-762. doi: 10.1182/blood-2018-09-876284. Epub 2018 Dec 13.
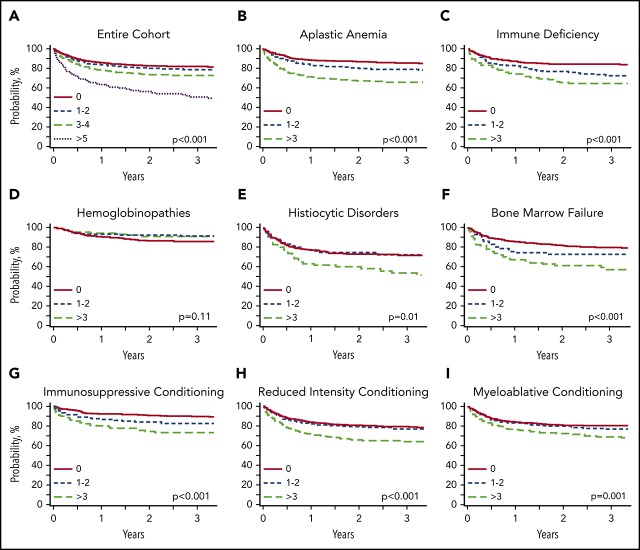
Despite improvements, mortality after allogeneic hematopoietic cell transplantation (HCT) for nonmalignant diseases remains a significant problem. We evaluated whether pre-HCT conditions defined by the HCT Comorbidity Index (HCT-CI) predict probability of posttransplant survival. Using the Center for International Blood and Marrow Transplant Research database, we identified 4083 patients with nonmalignant diseases transplanted between 2007 and 2014. Primary outcome was overall survival (OS) using the Kaplan-Meier method. Hazard ratios (HRs) were estimated by multivariable Cox regression models. Increasing HCT-CI scores translated to decreased 2-year OS of 82.7%, 80.3%, 74%, and 55.8% for patients with HCT-CI scores of 0, 1 to 2, 3 to 4, and ≥5, respectively, regardless of conditioning intensity. HCT-CI scores of 1 to 2 did not differ relative to scores of 0 (HR, 1.12 [95% CI, 0.93-1.34]), but HCT-CI of 3 to 4 and ≥5 posed significantly greater risks of mortality (HR, 1.33 [95% CI, 1.09-1.63]; and HR, 2.31 [95% CI, 1.79-2.96], respectively). The effect of HCT-CI differed by disease indication. Patients with acquired aplastic anemia, primary immune deficiencies, and congenital bone marrow failure syndromes with scores ≥3 had increased risk of death after HCT. However, higher HCT-CI scores among hemoglobinopathy patients did not increase mortality risk. In conclusion, this is the largest study to date reporting on patients with nonmalignant diseases demonstrating HCT-CI scores ≥3 that had inferior survival after HCT, except for patients with hemoglobinopathies. Our findings suggest that using the HCT-CI score, in addition to disease-specific factors, could be useful when developing treatment plans for nonmalignant diseases.
尽管有所改善,但异基因造血细胞移植(HCT)治疗非恶性疾病的死亡率仍然是一个重大问题。我们评估了 HCT 合并症指数(HCT-CI)定义的移植前状况是否预测移植后生存概率。我们使用国际血液和骨髓移植研究中心数据库,确定了 2007 年至 2014 年间接受非恶性疾病移植的 4083 名患者。主要结局是使用 Kaplan-Meier 方法的总生存率(OS)。通过多变量 Cox 回归模型估计风险比(HR)。无论预处理强度如何,HCT-CI 评分增加分别转化为 2 年 OS 降低 82.7%、80.3%、74%和 55.8%,患者的 HCT-CI 评分为 0、1-2、3-4 和≥5。HCT-CI 评分为 1-2 与评分为 0 没有差异(HR,1.12[95%CI,0.93-1.34]),但 HCT-CI 评分为 3-4 和≥5 死亡率的风险显著增加(HR,1.33[95%CI,1.09-1.63];和 HR,2.31[95%CI,1.79-2.96])。HCT-CI 的作用因疾病指征而异。HCT 后死亡风险增加的患者包括获得性再生障碍性贫血、原发性免疫缺陷和先天性骨髓衰竭综合征患者的 HCT-CI 评分为≥3,以及血红蛋白病患者的 HCT-CI 评分较高但不增加死亡率风险。总之,这是迄今为止报道最大的非恶性疾病患者研究,该研究显示 HCT-CI 评分为≥3 的患者在 HCT 后生存状况较差,除了血红蛋白病患者。我们的研究结果表明,除了血红蛋白病患者外,在制定非恶性疾病的治疗计划时,除了疾病特异性因素外,使用 HCT-CI 评分可能是有用的。