Anatomic Pathology, Department of Laboratory Medicine and Pathology, Mayo Clinic, 200 First Street, SW, Rochester, MN, 55905, USA.
Institute of Pathology, University Hospital Erlangen, Erlangen, Germany.
Acta Neuropathol. 2019 Feb;137(2):307-319. doi: 10.1007/s00401-018-1952-6. Epub 2018 Dec 24.
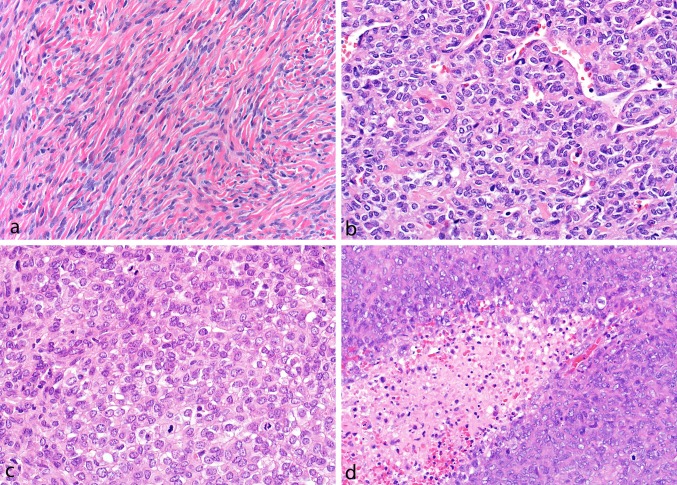
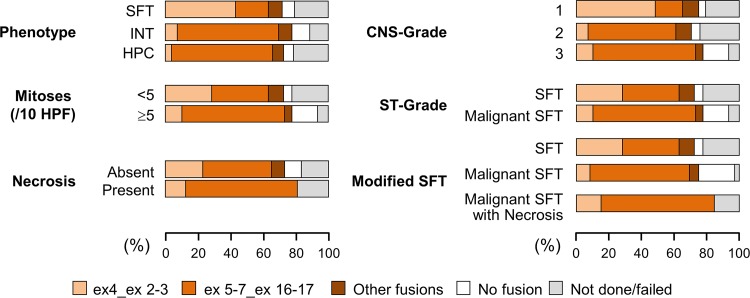
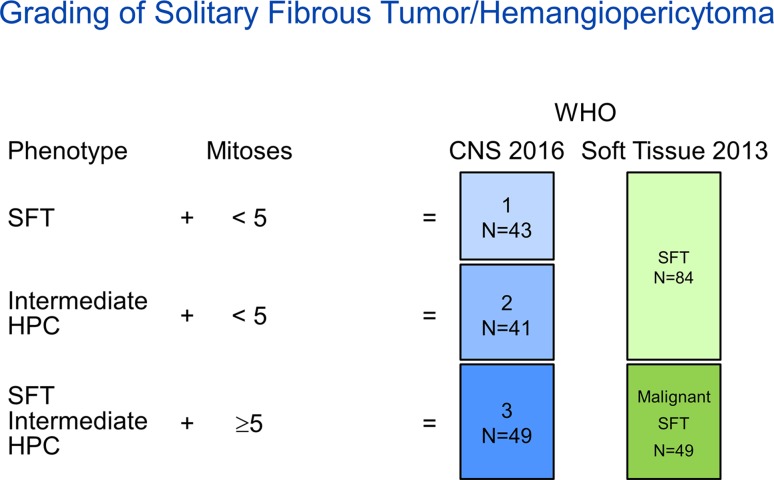
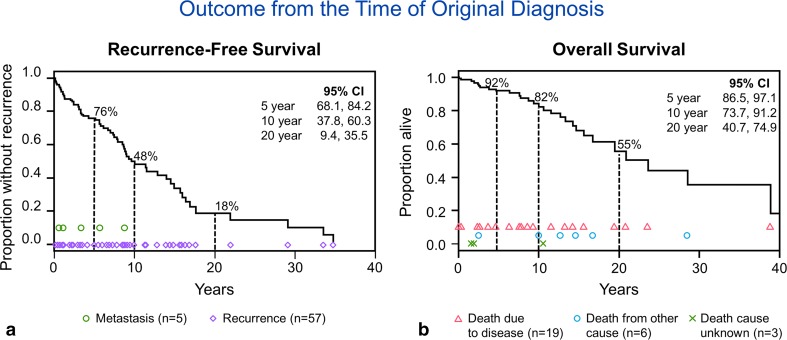
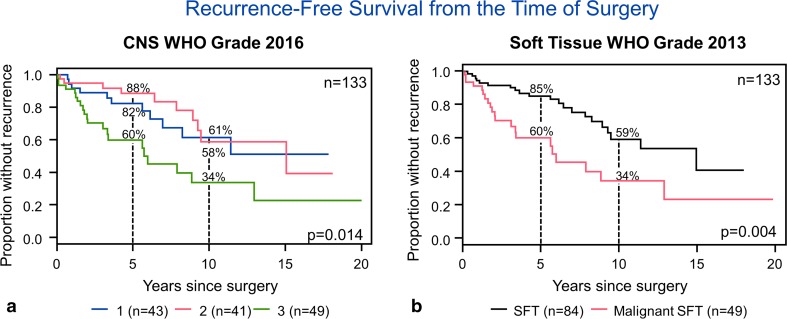
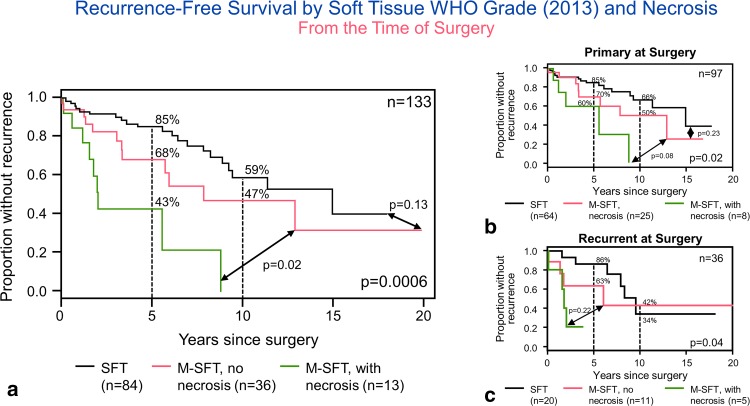
Meningeal solitary fibrous tumor (SFT)/hemangiopericytoma (HPC) is a rare tumor with propensity for recurrence and metastasis. Although multiple classification schemes have been proposed, optimal risk stratification remains unclear, and the prognostic impact of fusion status is uncertain. We compared the 2016 WHO CNS tumor grading scheme (CNS-G), a three-tier system based on histopathologic phenotype and mitotic count, to the 2013 WHO soft-tissue counterpart (ST-G), a two-tier system based on mitotic count alone, in a cohort of 133 patients [59 female, 74 male; mean age 54 years (range 20-87)] with meningeal SFT/HPC. Tumors were pathologically confirmed through review of the first tumor resection (n = 97), local recurrence (n = 35), or distant metastasis (n = 1). A STAT6 immunostain showed nuclear expression in 132 cases. NAB2-STAT6 fusion was detected in 99 of 111 successfully tested tumors (89%) including the single STAT6 immunonegative tumor. Tumors were classified by CNS-G as grade 1 (n = 43), 2 (n = 41), or 3 (n = 49), and by ST-G as SFT (n = 84) or malignant SFT (n = 49). Necrosis was present in 16 cases (12%). On follow-up, 42 patients had at least one subsequent recurrence or metastasis (7 metastasis only, 33 recurrence only, 2 patients had both). Twenty-nine patients died. On univariate analysis, necrosis (p = 0.002), CNS-G (p = 0.01), and ST-G (p = 0.004) were associated with recurrence-free (RFS) but not overall survival (OS). NAB2-STAT6 fusion type was not significantly associated with RFS or OS, but was associated with phenotype. A modified ST-G incorporating necrosis showed higher correlation with RFS (p = 0.0006) and remained significant (p = 0.02) when considering only the primary tumors. From our data, mitotic rate and necrosis appear to stratify this family of tumors most accurately and could be incorporated in a future grading scheme.
脑膜孤立性纤维瘤(SFT)/血管外皮细胞瘤(HPC)是一种罕见的肿瘤,具有复发和转移的倾向。尽管已经提出了多种分类方案,但最佳风险分层仍不清楚,融合状态的预后影响也不确定。我们比较了 2016 年世界卫生组织中枢神经系统肿瘤分级方案(CNS-G),这是一种基于组织病理学表型和有丝分裂计数的三级系统,与 2013 年世界卫生组织软组织对应方案(ST-G),这是一种仅基于有丝分裂计数的二级系统,在 133 例脑膜 SFT/HPC 患者[59 名女性,74 名男性;平均年龄 54 岁(范围 20-87 岁)]的队列中进行比较。通过对首次肿瘤切除术(n=97)、局部复发(n=35)或远处转移(n=1)的回顾性检查,对肿瘤进行病理确认。STAT6 免疫组化显示 132 例中有核表达。在 111 例成功检测的肿瘤中,检测到 99 例 NAB2-STAT6 融合(89%),包括单例 STAT6 免疫阴性肿瘤。根据 CNS-G 分类,肿瘤为 1 级(n=43)、2 级(n=41)或 3 级(n=49),根据 ST-G 分类为 SFT(n=84)或恶性 SFT(n=49)。16 例存在坏死(12%)。在随访中,42 例至少有一次后续复发或转移(7 例仅有转移,33 例仅有复发,2 例两者兼有)。29 例患者死亡。单因素分析显示,坏死(p=0.002)、CNS-G(p=0.01)和 ST-G(p=0.004)与无复发生存(RFS)相关,但与总生存(OS)无关。NAB2-STAT6 融合类型与 RFS 或 OS 无显著相关性,但与表型相关。纳入坏死的改良 ST-G 与 RFS 的相关性更高(p=0.0006),仅考虑原发性肿瘤时仍具有显著意义(p=0.02)。根据我们的数据,有丝分裂率和坏死似乎最能准确地对这类肿瘤进行分层,并且可以纳入未来的分级方案中。