Wen Ying-Sheng, Xi Ke-Xing, Xi Ke-Xiang, Zhang Ru-Si, Wang Gong-Ming, Huang Zi-Rui, Zhang Lan-Jun
State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, People's Republic of China,
Department of Thoracic Surgery, Sun Yat-sen University Cancer Center, Guangzhou 510060, People's Republic of China.
Cancer Manag Res. 2018 Dec 12;10:6869-6877. doi: 10.2147/CMAR.S186047. eCollection 2018.
For the patients with pathologic T2 N0 non-small cell lung cancer (NSCLC), the extent of lymph node (LN) removal required for survival is controversial. We aimed to explore the prognostic significance of examined LNs and to identify how many nodes should be examined.
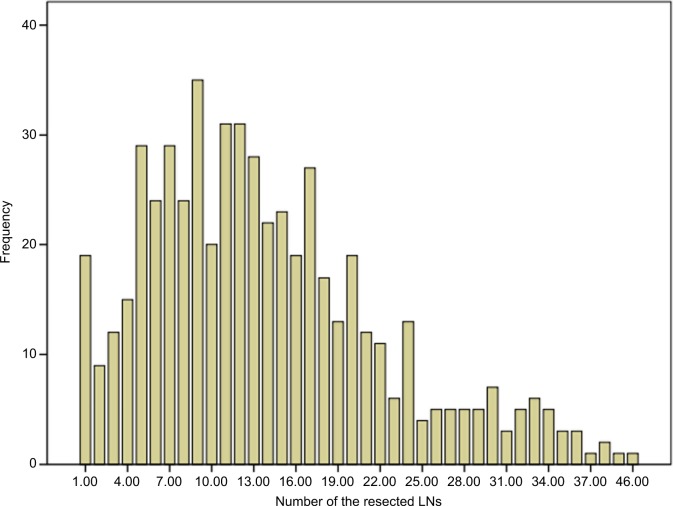
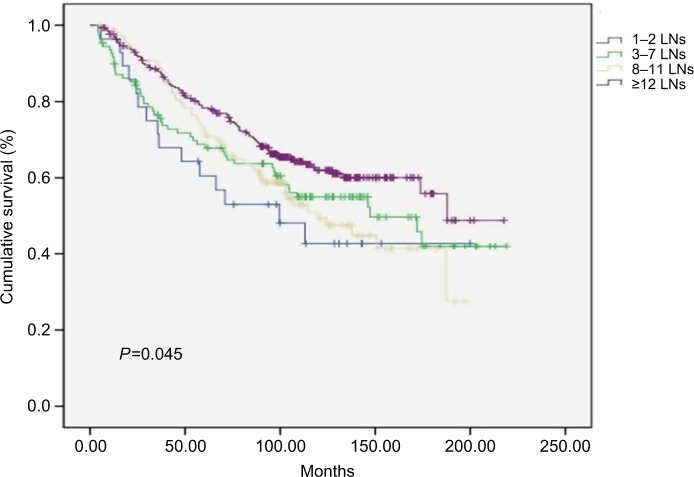
We reviewed 549 patients who underwent pulmonary or pneumonectomy surgery or plus lymphadenectomy who were confirmed as T2 stage and LN negative by postoperative pathological diagnosis. According to Martingale residuals of the Cox model, the patients were classified into four groups by the number of examined LNs (1-2 LNs, 3-7 LNs, 8-11 LNs, and ≥12 LNs). Kaplan-Meier analysis and Cox regression analysis were used to evaluate the association between survival and the number of examined LNs.
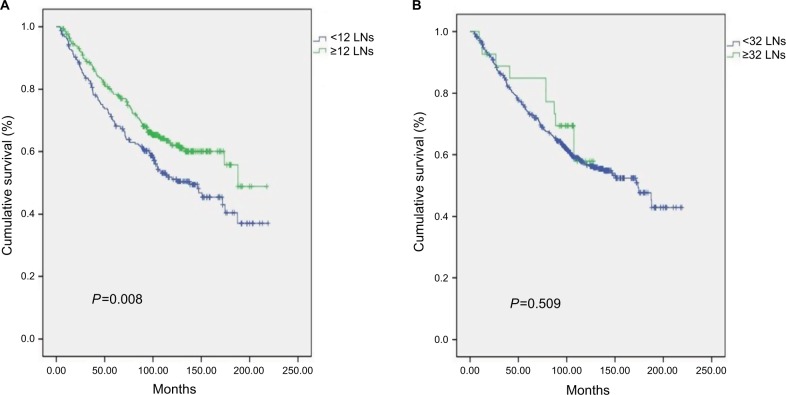
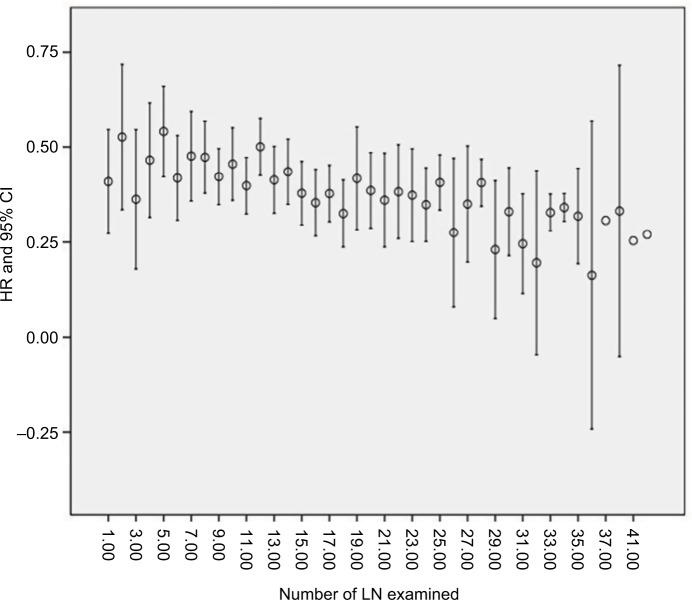
Compared with the 1-2 LNs, 3-7 LNs, and 8-11 LNs groups, the survival was significantly better in the ≥12 LNs group. The 5-year cancer-specific survival rate was 60.5% for patients with 1-2 negative LNs, compared with 68.7%, 72.6%, and 78.4% for those with 3-7, 8-11, and >11 LNs examined, respectively. The 7-year cancer-specific survival rate was 52.9% for patients with 1-2 negative LNs, compared with 63.7%, 63.8%, and 70.8% for those with 3-7, 8-11, and >11 LNs examined, respectively (=0.045). There was a significant drop in mortality risk with the examination of more LNs. The lowest mortality risk occurred in those with 32 or more LNs examined. Multivariate analysis showed that age and the number of examined LNs were strong independent predictors of survival.
The number of examined LNs is a strong independent prognostic factor. Our study demonstrates that patients with T2 N0 NSCLC should have at least 12 LNs examined and that the results of this study may provide information for the optimal number of resected LNs in surgery.
对于病理分期为T2 N0的非小细胞肺癌(NSCLC)患者,为求生存所需的淋巴结(LN)清扫范围存在争议。我们旨在探讨送检LN的预后意义,并确定应检查多少个淋巴结。
我们回顾了549例行肺切除术或全肺切除术或加淋巴结清扫术的患者,这些患者术后病理诊断确诊为T2期且LN阴性。根据Cox模型的鞅残差,将患者按送检LN数量分为四组(1 - 2个LN、3 - 7个LN、8 - 11个LN和≥12个LN)。采用Kaplan - Meier分析和Cox回归分析来评估生存率与送检LN数量之间的关联。
与1 - 2个LN、3 - 7个LN和8 - 11个LN组相比,≥12个LN组的生存率显著更高。1 - 2个阴性LN患者的5年癌症特异性生存率为60.5%,而送检3 - 7个、8 - 11个和>11个LN的患者分别为68.7%、72.6%和78.4%。1 - 2个阴性LN患者的7年癌症特异性生存率为52.9%,而送检3 - 7个、8 - 11个和>11个LN的患者分别为63.7%、63.8%和70.8%(P = 0.045)。检查更多的LN,死亡风险显著下降。检查32个或更多LN的患者死亡风险最低。多因素分析表明,年龄和送检LN数量是生存的强有力独立预测因素。
送检LN数量是一个强有力的独立预后因素。我们的研究表明,T2 N0 NSCLC患者应至少检查12个LN,本研究结果可为手术中切除LN的最佳数量提供信息。