Hu Fang-Bin, Cui Lian-Qun
Department of Cardiology, Provincial Hospital Affiliated to Shandong University, Jinan, Shandong 250021, China.
Department of Cardiology, Jingjiang People's Hospital, Jingjiang, Jiangsu 214500, China.
Chronic Dis Transl Med. 2018 Apr 12;4(4):260-267. doi: 10.1016/j.cdtm.2017.11.002. eCollection 2018 Dec.
Although controversial, the intra-aortic balloon pump (IABP) and percutaneous left ventricular assist device (PLVAD) are widely used for initial hemodynamic stabilization. We performed a meta-analysis to compare the clinical outcomes of these two devices in patients with severe left ventricular (LV) dysfunction undergoing percutaneous coronary intervention (PCI) or ventricular tachycardia (VT) ablation.
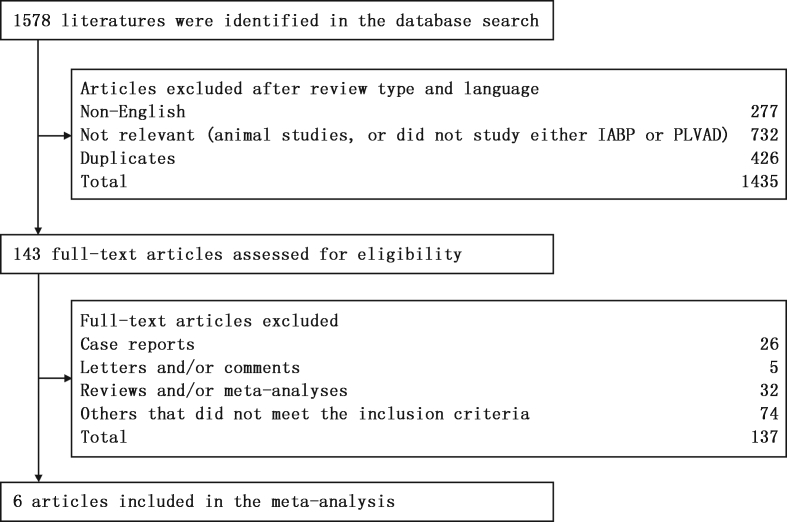
MEDLINE, EMBASE, the Cochrane Registry of Controlled Trials, and reference lists of relevant articles were searched. We included randomized controlled trials (RCTs) and prospective observational studies. Meta-analysis was conducted using a random effects model.
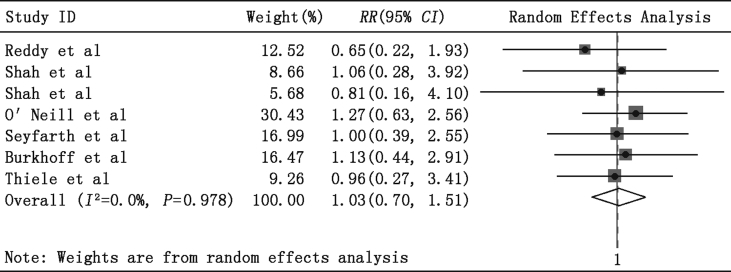
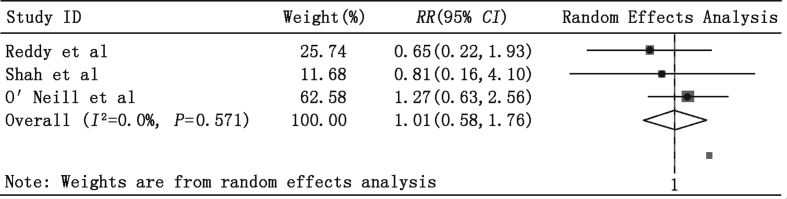
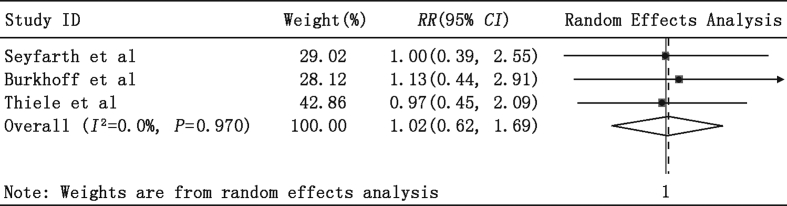
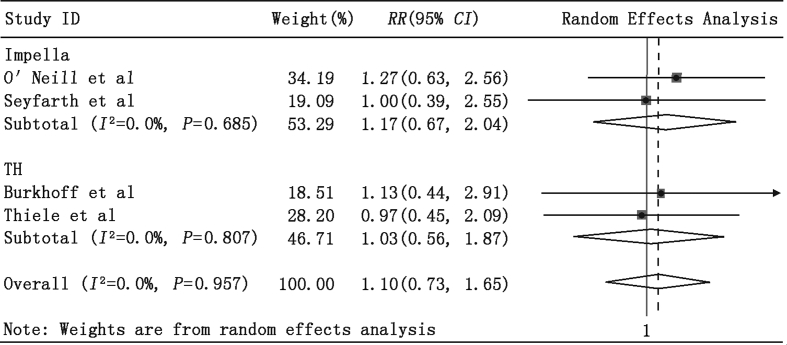
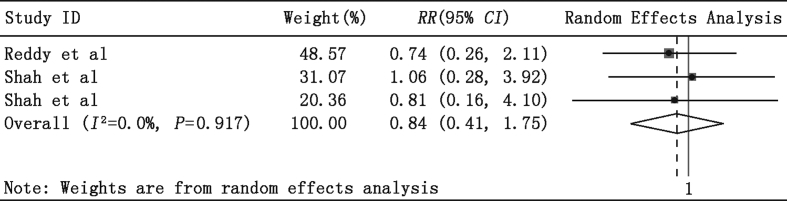
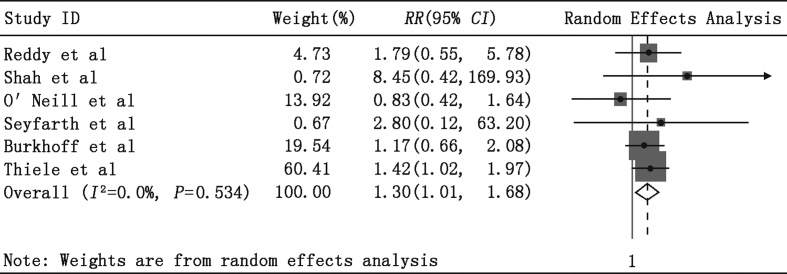
The quantitative analysis included 4 RCTs and 2 observational studies. A total of 348 patients received PLVAD and 340 received IABP. Meta-analysis revealed that early mortality rates (in-hospital or 30-day) did not differ between the PLVAD and IABP groups (relative risk () = 1.03, 95% confidence interval () = 0.70-1.51, = 0.89). Significant differences were observed between the two groups in the composite, in-hospital, non-major adverse cardiac and cerebrovascular events (MACCE) rate ( = 1.30, 95% = 1.01-1.68, = 0.04).
Compared with IABP, PLVAD with active circulatory support did not improve early survival in those with severe left ventricular dysfunction undergoing either PCI or VT ablation, but increased the in-hospital non-MACCE rate.
尽管存在争议,但主动脉内球囊反搏(IABP)和经皮左心室辅助装置(PLVAD)仍被广泛用于初始血流动力学稳定。我们进行了一项荟萃分析,以比较这两种装置在接受经皮冠状动脉介入治疗(PCI)或室性心动过速(VT)消融的严重左心室(LV)功能障碍患者中的临床结局。
检索了MEDLINE、EMBASE、Cochrane对照试验注册库以及相关文章的参考文献列表。我们纳入了随机对照试验(RCT)和前瞻性观察性研究。使用随机效应模型进行荟萃分析。
定量分析包括4项RCT和2项观察性研究。共有348例患者接受了PLVAD,340例接受了IABP。荟萃分析显示,PLVAD组和IABP组的早期死亡率(住院期间或30天)无差异(相对危险度(RR)=1.03,95%置信区间(CI)=0.70-1.51,P=0.89)。两组在综合住院期间非重大不良心脑血管事件(MACCE)发生率方面存在显著差异(RR=1.30,95%CI=1.01-1.68,P=0.04)。
与IABP相比,具有主动循环支持的PLVAD在接受PCI或VT消融的严重左心室功能障碍患者中并未改善早期生存率,但增加了住院期间非MACCE发生率。