Division of Infectious Diseases & International Medicine, University of Minnesota, Minnesota, United States of America.
Infectious Diseases Institute, Makerere University, Kampala, Uganda.
PLoS One. 2019 Jan 10;14(1):e0210105. doi: 10.1371/journal.pone.0210105. eCollection 2019.
Cryptococcal meningitis accounts for 15% of AIDS-related mortality. Cryptococcal antigen (CrAg) is detected in blood weeks before onset of meningitis, and CrAg positivity is an independent predictor of meningitis and death. CrAg screening for patients with advanced HIV and preemptive treatment is recommended by the World Health Organization, though implementation remains limited. Our objective was to evaluate costs and mortality reduction (lives saved) from a national CrAg screening program across Uganda.
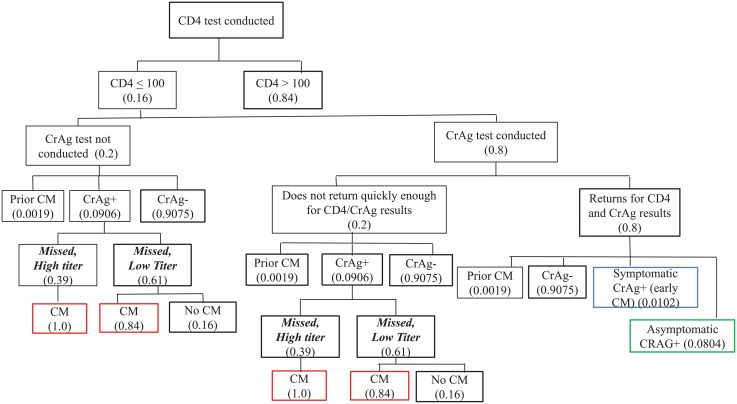
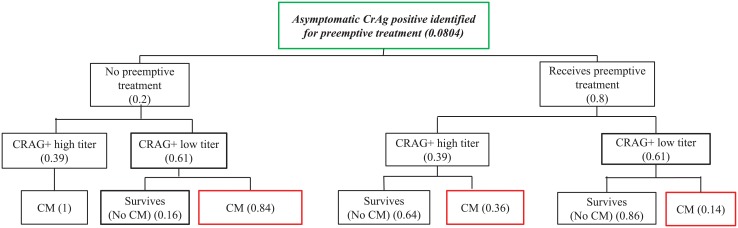
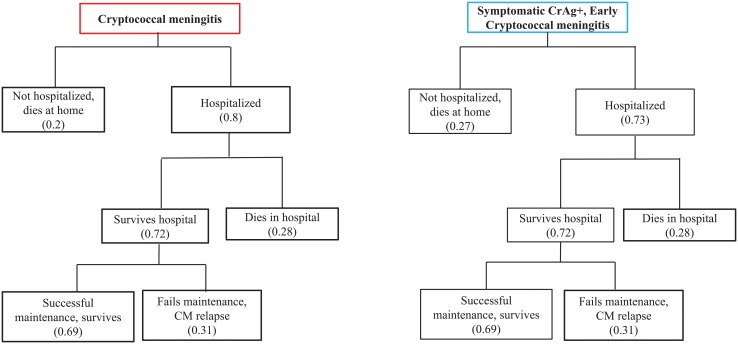
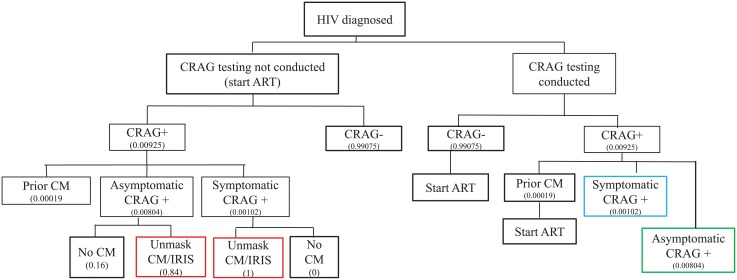
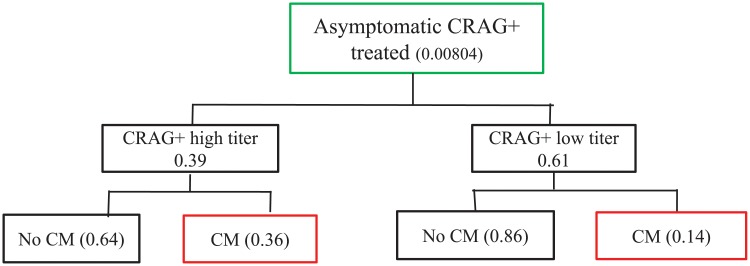
We created a decision analytic model to evaluate CrAg screening. CrAg screening was considered for those with a CD4<100 cells/μL per national and international guidelines, and in the context of a national HIV test-and-treat program where CD4 testing was not available. Costs (2016 USD) were estimated for screening, preemptive therapy, hospitalization, and maintenance therapy. Parameter assumptions were based on large prospective CrAg screening studies in Uganda, and clinical trials from sub Saharan Africa. CrAg positive (CrAg+) persons could be: (a) asymptomatic and thus eligible for preemptive treatment with fluconazole; or (b) symptomatic with meningitis with hospitalization.
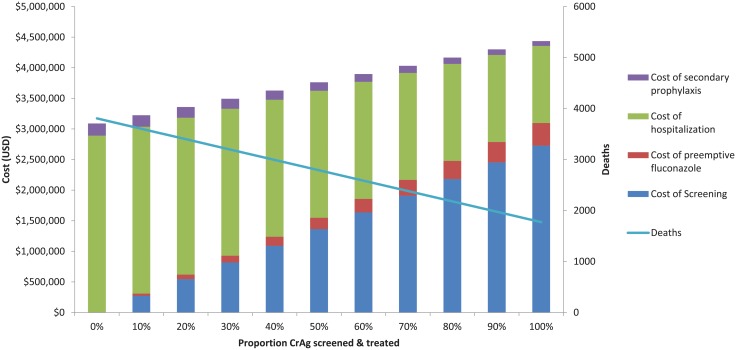
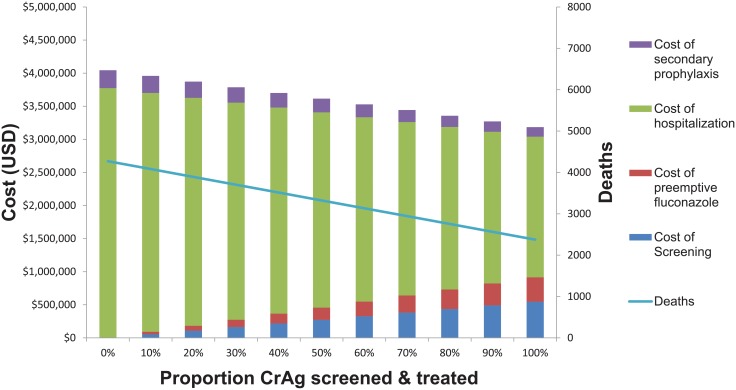
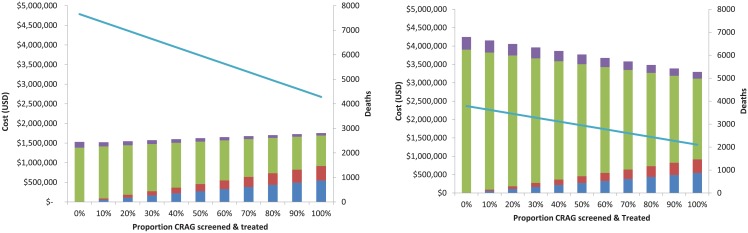
In the base case model for 1 million persons with a CD4 test annually, 128,000 with a CD4<100 cells/μL were screened, and 8,233 were asymptomatic CrAg+ and received preemptive therapy. Compared to no screening and treatment, CrAg screening and treatment in the base case cost $3,356,724 compared to doing nothing, and saved 7,320 lives, for a cost of $459 per life saved, with the $3.3 million in cost savings derived from fewer patients developing fulminant meningitis. In the scenario of a national HIV test-and-treat program, of 1 million HIV-infected persons, 800,000 persons were screened, of whom 640,000 returned to clinic, and 8,233 were incident CrAg positive (CrAg prevalence 1.4%). The total cost of a CrAg screening and treatment program was $4.16 million dollars, with 2,180 known deaths. Conversely, without CrAg screening, the cost of treating meningitis was $3.09 million dollars with 3,806 deaths. Thus, despite the very low CrAg prevalence of 1.4% in the general HIV-infected population, and inadequate retention-in-care, CrAg screening averted 43% of deaths from cryptococcal meningitis at a cost of $662 per death averted.
CrAg screening and treatment programs are cost-saving and lifesaving, assuming preemptive treatment is 77% effective in preventing death, and could be adopted and implemented by ministries of health to reduce mortality in those with advanced HIV disease. Even within HIV test-and-treat programs where CD4 testing is not performed, and CrAg prevalence is only 1.4%, CrAg screening is cost-effective.
隐球菌性脑膜炎占艾滋病相关死亡人数的 15%。隐球菌抗原 (CrAg) 在脑膜炎发病前数周即可在血液中检测到,CrAg 阳性是脑膜炎和死亡的独立预测因素。世界卫生组织建议对晚期艾滋病患者进行隐球菌抗原筛查,并进行预防性治疗,尽管实施情况仍然有限。我们的目的是评估乌干达全国性隐球菌抗原筛查计划的成本和死亡率降低(挽救生命)。
我们创建了一个决策分析模型来评估隐球菌抗原筛查。根据国家和国际指南,对于 CD4 细胞<100 个/μL 的患者,以及在国家艾滋病毒检测和治疗方案中无法进行 CD4 检测的情况下,考虑进行隐球菌抗原筛查。(2016 年美元)用于筛查、预防性治疗、住院和维持治疗的成本进行了估算。参数假设基于乌干达的大型前瞻性隐球菌抗原筛查研究和撒哈拉以南非洲的临床试验。隐球菌抗原阳性(CrAg+)的人可能为:(a)无症状,因此有资格接受氟康唑预防性治疗;或(b)有症状的脑膜炎患者,需要住院治疗。
在每年有 100 万人接受 CD4 检测的基础病例模型中,有 128000 人 CD4 细胞<100 个/μL,其中 8233 人无症状 CrAg+并接受了预防性治疗。与不筛查和治疗相比,筛查和治疗在基础病例中花费了 335.6724 万美元,而不做任何事情则花费了 3356.724 万美元,挽救了 7320 条生命,每挽救一条生命的成本为 459 美元,节省的 330 万美元来自于减少更多的患者发生暴发性脑膜炎。在全国艾滋病毒检测和治疗方案的情况下,对于 100 万艾滋病毒感染者,有 80 万人接受了筛查,其中 64 万人返回诊所,有 8233 人新出现隐球菌抗原阳性(隐球菌抗原阳性率为 1.4%)。隐球菌抗原筛查和治疗计划的总成本为 416 万美元,已知有 2180 人死亡。相反,如果不进行隐球菌抗原筛查,治疗脑膜炎的费用为 3090 万美元,死亡人数为 3806 人。因此,尽管在一般艾滋病毒感染人群中隐球菌抗原的患病率仅为 1.4%,而且保留治疗的情况不足,但隐球菌抗原筛查以每例死亡成本 662 美元的成本避免了 43%的隐球菌性脑膜炎死亡。
假设预防性治疗在预防死亡方面的有效性为 77%,隐球菌抗原筛查和治疗方案可以节省成本并挽救生命,并且可以被卫生部门采用和实施,以降低晚期艾滋病患者的死亡率。即使在不进行 CD4 检测且隐球菌抗原患病率仅为 1.4%的艾滋病毒检测和治疗方案中,隐球菌抗原筛查也是具有成本效益的。