Institute of Gerontology and Geriatrics, Santa Maria della Misericordia Hospital, Department of Medicine, University of Perugia, 06123 Perugia PG, Italy.
Nutrients. 2019 Jan 9;11(1):128. doi: 10.3390/nu11010128.
Hypovitaminosis D is a frequent condition in elderly subjects. Vitamin D adequacy is best determined by measurement of the 25-hydroxyvitamin D-25(OH)D-concentration in the serum. An inverse association exists between 25(OH)D and cardiovascular, infectious, glucose metabolism, cognitive disorders, and all-cause mortality. Whether 25(OH)D is a marker of organ diseases is still under debate. We aimed to investigate whether comorbidities were associated with serum 25(OH)D levels in geriatric inpatients.
This is a retrospective study, including 237 subjects consecutively admitted to an acute care geriatric unit, with available data of 25(OH)D serum concentrations. 25(OH)D serum levels were defined according to the following cutoffs: 50⁻30 ng/mL (125⁻75 nmol/L): optimal range; 30⁻20 ng/mL (75⁻50 nmol/L): insufficiency; 20⁻10 ng/mL (5⁻25 nmol/L): deficiency; and <10 ng/mL (<25 nmol/L): severe deficiency. Comorbidity was assessed using the Cumulative Illness Rating Scale-Geriatric (CIRS-G). Two summary measures were obtained, the Illness Severity Index (CIRS-SI) and the Comorbidity Index (CIRS-CI).
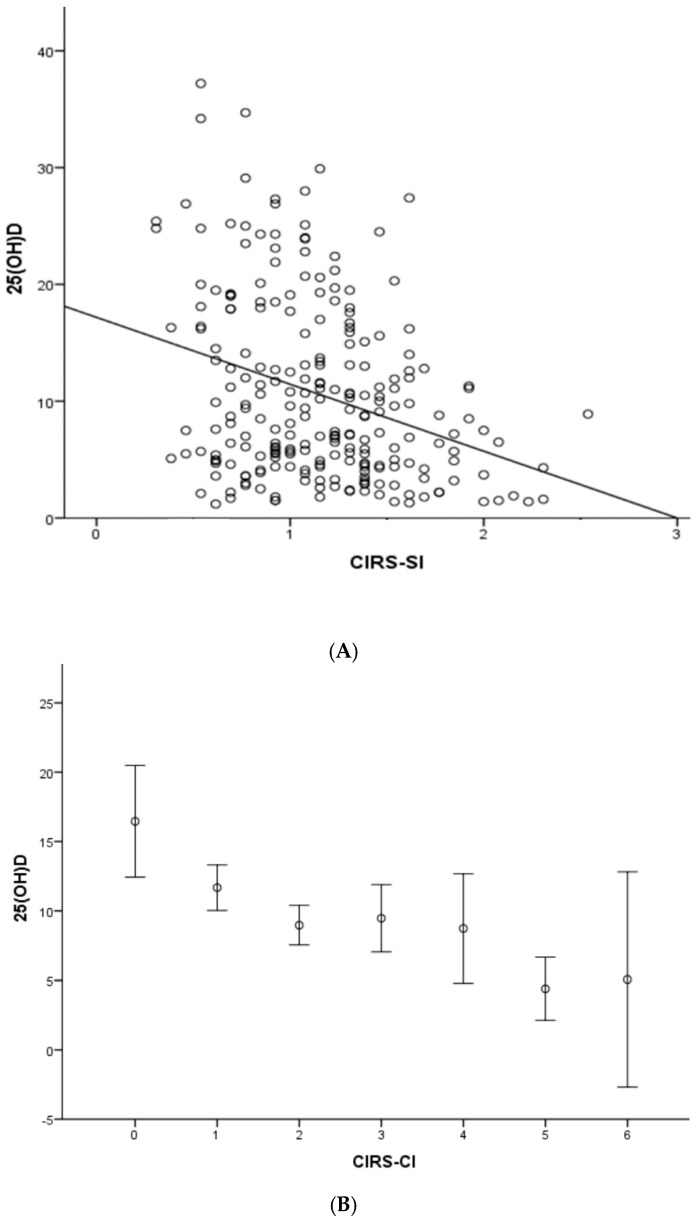
177 (74.68%) women and 60 (25.32%) men with mean age of 85 ± 6 years old were enrolled. The majority of subjects (68.6%) were at risk of malnutrition. Overall, the burden of comorbidity was 1.87 ± 1.33 for CIRS-CI and 1.18 ± 0.40 for CIRS-SI. 25(OH)D serum concentrations were 10.58 ± 7.68 ng/mL, with 98.7% of subjects having vitamin D below 30 ng/mL and 56.6% with severe deficiency. An inverse correlation was found between 25(OH)D and both CIRS-SI (: -0.312; < 0.0001) and CIRS-CI (: -0.306; < 0.0001). Independent of multiple covariates an inverse association between both CIRS-SI ( < 0.0001) and CIRS-CI ( < 0.0001) and 25(OH)D was confirmed. Both CIRS-SI ( = 0.251, < 0.0001) and CIRS-CI ( = 0.137, = 0.016) were positively correlated with the length of hospital stay. An inverse correlation was confirmed between serum 25(OH)D concentrations and CRP ( = -0.142; = 0.041). CRP, in turn, positively correlated with CIRS-SI ( = 0.209, = 0.003) and CIRS-CI ( = 0.158, = 0.023). Both CIRS-SI ( = 0.251, < 0.0001) and CIRS-CI ( = 0.137, = 0.016) were positively correlated with the length of hospital stay.
In hospitalized very old subjects, a higher comorbidity burden is associated with lower 25(OH)D serum levels. Hypovitaminosis D was correlated with higher inflammatory status, which, together with the comorbidities burden, negatively influenced the length of hospital stay.
维生素 D 不足在老年人群中很常见。血清 25-羟维生素 D-25(OH)D 浓度的测定是确定维生素 D 充足的最佳方法。25(OH)D 与心血管疾病、传染病、葡萄糖代谢、认知障碍和全因死亡率呈负相关。25(OH)D 是否是器官疾病的标志物仍存在争议。我们旨在研究老年住院患者的合并症是否与血清 25(OH)D 水平相关。
这是一项回顾性研究,包括连续收治于急性护理老年病房的 237 例患者,这些患者均有 25(OH)D 血清浓度的数据。根据以下切点定义 25(OH)D 血清水平:50-30ng/ml(125-75nmol/L):最佳范围;30-20ng/ml(75-50nmol/L):不足;20-10ng/ml(5-25nmol/L):缺乏;<10ng/ml(<25nmol/L):严重缺乏。使用累积疾病评分量表-老年版(CIRS-G)评估合并症。获得两个综合指标,疾病严重程度指数(CIRS-SI)和合并症指数(CIRS-CI)。
共纳入 177 名(74.68%)女性和 60 名(25.32%)男性,平均年龄 85±6 岁。大多数患者(68.6%)存在营养不良风险。总的来说,CIRS-CI 的合并症负担为 1.87±1.33,CIRS-SI 为 1.18±0.40。25(OH)D 血清浓度为 10.58±7.68ng/ml,98.7%的患者维生素 D 水平低于 30ng/ml,56.6%的患者存在严重缺乏。25(OH)D 与 CIRS-SI(:-0.312;<0.0001)和 CIRS-CI(:-0.306;<0.0001)呈负相关。在调整了多个协变量后,CIRS-SI(<0.0001)和 CIRS-CI(<0.0001)与 25(OH)D 之间仍然存在负相关。CIRS-SI(=0.251,<0.0001)和 CIRS-CI(=0.137,=0.016)均与住院时间呈正相关。血清 25(OH)D 浓度与 CRP(=−0.142;=0.041)呈负相关。CRP 与 CIRS-SI(=0.209,=0.003)和 CIRS-CI(=0.158,=0.023)呈正相关。CIRS-SI(=0.251,<0.0001)和 CIRS-CI(=0.137,=0.016)均与住院时间呈正相关。
在住院的高龄患者中,合并症负担越重,25(OH)D 血清水平越低。维生素 D 不足与更高的炎症状态相关,而炎症状态和合并症负担都会对住院时间产生负面影响。