Urrutia Liceth Carolina, Patiño-Barbosa Andrés Mauricio, Arroyave-Valencia Felipe, Sabogal-Roman Juan Alejandro, Cardona-Ospina Jaime A, Rodriguez-Morales Alfonso J
Epidemiology and Public Health, Universidad Tecnológica De Pereira, Pereira, COL.
Cureus. 2018 Oct 31;10(10):e3528. doi: 10.7759/cureus.3528.
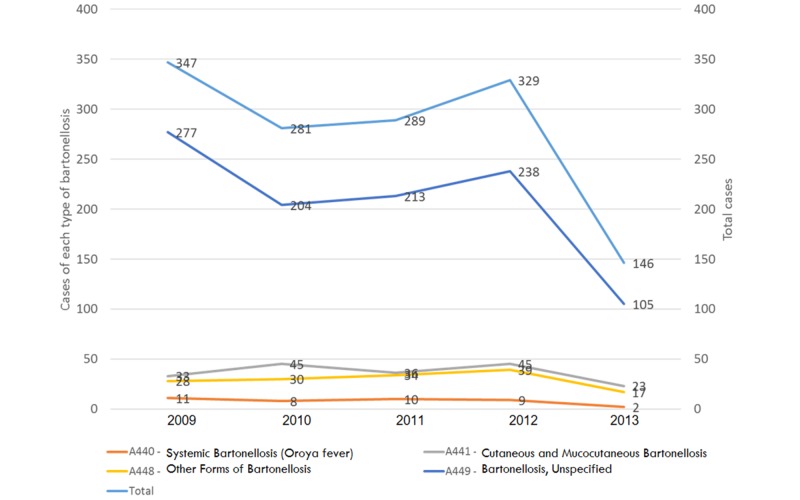
Background , the etiological agent of Carrion's disease and presumed to be transmitted by phlebotomine sandflies, is endemic to the high-altitude valleys of the South American Andes, including Colombia. Methods This observational, retrospective study in which the incidence of bartonelloses (International Classification of Diseases, 10th revision (ICD-10) codes A44.0-A44.9) in Colombia, from 2009-2013, was estimated based on data extracted from the personal health records system (, RIPS). Using the official population estimates of the National Statistics Department (, DANE), crude and adjusted incidence rates were estimated (cases/100,000 population). Results A total of 1,389 cases were reported (median 289/year), for a cumulative national rate of 3.02 cases/100,000 population; 91.2% were female; 66.8% were <40-year-old (3.8% <9.9-year-old). The cases were 2.9% Oroya fever (A44.0), 13.1% verruga peruana (A44.1), and the rest (85.3%) were other forms of bartonelloses (A44.8-A44.9). The highest rates of Oroya fever were reported in Bolivar (2.5 cases/1,000,000 population). For verruga peruana highest number of cases were reported in Antioquia (32; 17.8%; 5.21 cases/1,000,000 population) and the highest rate at Magdalena (11.54 cases/1,000,000 population) (Risaralda, 6.45; Caldas, 5.1). For other forms of bartonelloses, the highest rates were reported at Magdalena (48.65 cases/1,000,000 population), followed by Huila (32.8) and La Guajira (18.9). At Nariño, Putumayo, Amazonas, Cauca, and Valle del Cauca, 11.7% of the cases of the country were reported. Conclusions the potential vector of in Colombia, is distributed not only in Nariño, Cauca, and Valle del Cauca but also in the Antioquia, Caldas, Huila, La Guajira, Risaralda, Cordoba, and Caribbean areas. Given this distribution, the transmission would be occurring, as seen in reported cases, in more areas than previously described by classic reports of these diseases in the country.
卡里翁病的病原体被认为是通过白蛉传播的,在包括哥伦比亚在内的南美洲安第斯山脉的高海拔山谷地区呈地方性流行。方法:这项观察性回顾性研究基于从个人健康记录系统(RIPS)提取的数据,估计了2009年至2013年哥伦比亚巴尔通体病(国际疾病分类第10版(ICD - 10)编码A44.0 - A44.9)的发病率。利用国家统计局(DANE)的官方人口估计数,估算了粗发病率和调整发病率(病例数/10万人口)。结果:共报告1389例(中位数为每年289例),全国累计发病率为3.02例/10万人口;91.2%为女性;66.8%年龄小于40岁(3.8%年龄小于9.9岁)。病例中奥罗亚热(A44.0)占2.9%,秘鲁疣(A44.1)占13.1%,其余(85.3%)为其他形式的巴尔通体病(A44.8 - A44.9)。奥罗亚热发病率最高的是玻利瓦尔省(2.5例/100万人口)。秘鲁疣报告病例数最多的是安蒂奥基亚省(32例;17.8%;5.21例/100万人口),马格达莱纳省发病率最高(11.54例/100万人口)(里萨拉尔达省为6.45例;卡尔达斯省为5.1例)。对于其他形式的巴尔通体病,发病率最高的是马格达莱纳省(48.65例/100万人口),其次是乌伊拉省(32.8例)和瓜希拉省(18.9例)。纳里尼奥省、普图马约省、亚马孙省、考卡省和考卡山谷省报告了该国11.7%的病例。结论:哥伦比亚的潜在传播媒介不仅分布在纳里尼奥省、考卡省和考卡山谷省,还分布在安蒂奥基亚省、卡尔达斯省、乌伊拉省、瓜希拉省、里萨拉尔达省、科尔多瓦省和加勒比地区。鉴于这种分布情况,正如报告病例所示,传播发生的地区比该国这些疾病的经典报告中先前描述的更多。