Philadelphia FIGHT, 1233 Locust Street, 5th floor, Philadelphia, PA, 19107, USA.
AIDS Healthcare Foundation, 352 7th Ave., STE 1205, New York, NY, 10001, USA.
AIDS Res Ther. 2019 Jan 16;16(1):1. doi: 10.1186/s12981-019-0217-3.
HLA-B57:01 screening was added to clinical care guidelines in 2008 to reduce the risk of hypersensitivity reaction from abacavir. The uptake of HLA-B57:01 screening and incidence of hypersensitivity reaction were assessed in a prospective clinical cohort in the United States to evaluate the effectiveness of this intervention.
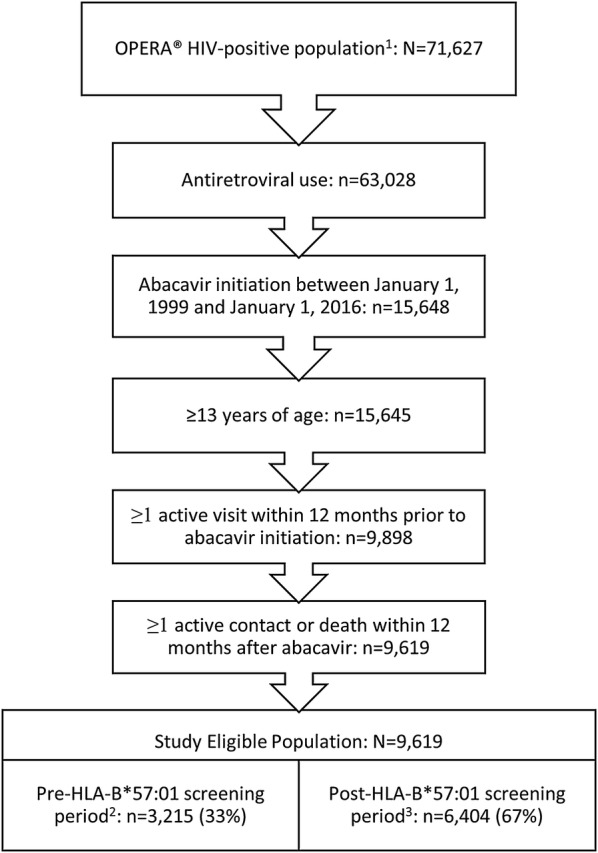
We included all patients initiating an abacavir-containing regimen for the first time in the pre-HLA-B57:01 screening period (January 1, 1999 to June 14, 2008) or the post-HLA-B57:01 screening period (June 15, 2008 to January 1, 2016). Yearly incidence of both HLA-B*57:01 screening and physician panel-adjudicated hypersensitivity reactions were calculated and compared.
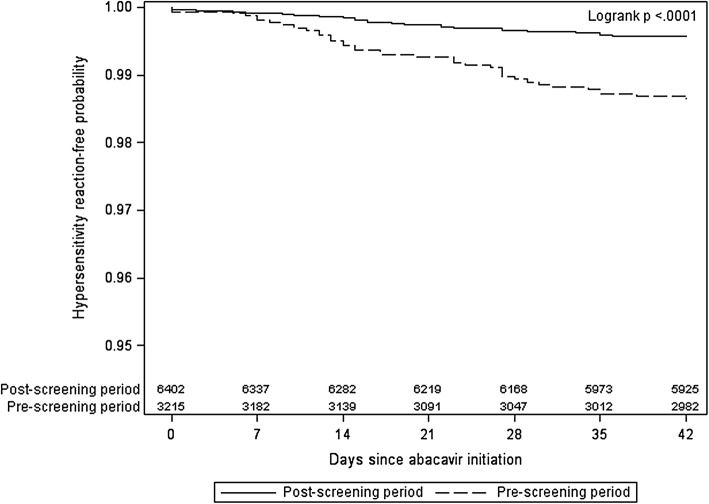
Of the 9619 patients eligible for the study, 33% initiated abacavir in the pre-screening period and 67% in the post-screening period. Incidence of HLA-B*57:01 screening prior to abacavir initiation increased from 43% in 2009 to 84% in 2015. The incidence of definite or probable hypersensitivity reactions decreased from 1.3% in the pre-screening period to 0.8% in 2009 and further to 0.2% in 2015 in the post-screening period.
Frequency of HLA-B57:01 screening increased steadily since its first inclusion in treatment guidelines in the United States. This increase in screening was accompanied by a decreasing incidence of definite or probable hypersensitivity reactions over the same period. However, a considerable proportion of patients initiating abacavir were not screened, representing a failed opportunity to prevent hypersensitivity reactions. Where HLA-B57:01 screening is standard of care, patients should be confirmed negative for this allele before starting abacavir treatment.
2008 年,为降低阿巴卡韦引起的过敏反应风险,HLA-B57:01 筛查被纳入临床护理指南。本研究通过在美国开展的前瞻性临床队列评估 HLA-B57:01 筛查的实施情况和过敏反应的发生率,以评估该干预措施的有效性。
我们纳入了在 HLA-B57:01 筛查前(1999 年 1 月 1 日至 2008 年 6 月 14 日)或后(2008 年 6 月 15 日至 2016 年 1 月 1 日)首次使用含阿巴卡韦方案的所有患者。计算并比较了每年 HLA-B57:01 筛查和经医生专家组裁决的过敏反应的发生率。
在符合研究条件的 9619 例患者中,33%的患者在筛查前接受阿巴卡韦治疗,67%的患者在筛查后接受阿巴卡韦治疗。阿巴卡韦治疗前 HLA-B*57:01 筛查的发生率从 2009 年的 43%增加到 2015 年的 84%。筛查前确定或可能的过敏反应发生率从 1.3%降至 2009 年的 0.8%,再降至 2015 年筛查后的 0.2%。
自美国首次将 HLA-B57:01 筛查纳入治疗指南以来,其筛查频率稳步上升。在此期间,筛查的增加伴随着确定或可能的过敏反应发生率的降低。然而,相当一部分开始使用阿巴卡韦的患者未接受筛查,这代表着预防过敏反应的机会错失。在 HLA-B57:01 筛查成为标准护理的情况下,在开始阿巴卡韦治疗前应确认患者 HLA-B*57:01 等位基因阴性。