Lee Julia, Shukla Dave R, Sánchez-Sotelo Joaquín
Department of Orthopaedic Surgery, Mayo Clinic, Rochester, MN, USA.
JSES Open Access. 2018 Mar 1;2(1):74-83. doi: 10.1016/j.jses.2017.11.006. eCollection 2018 Mar.
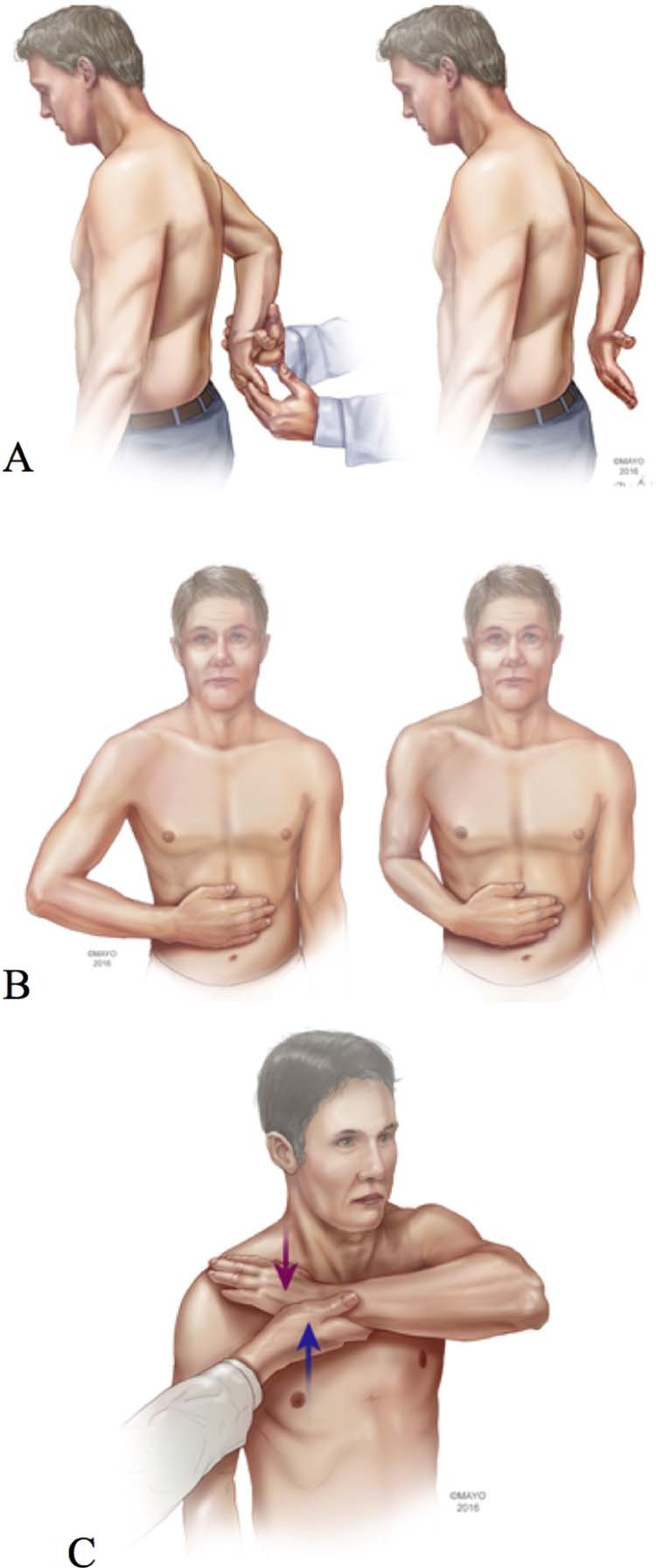
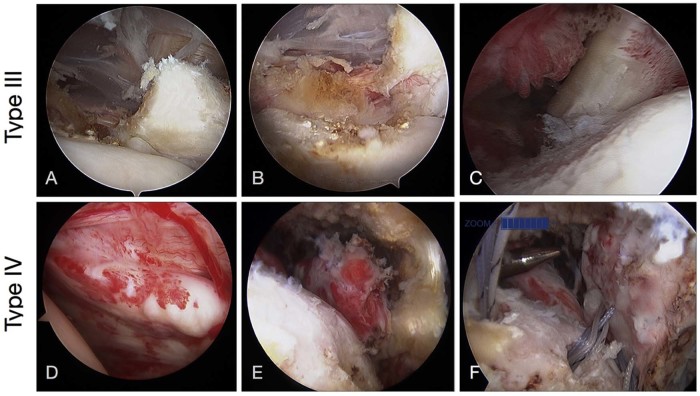
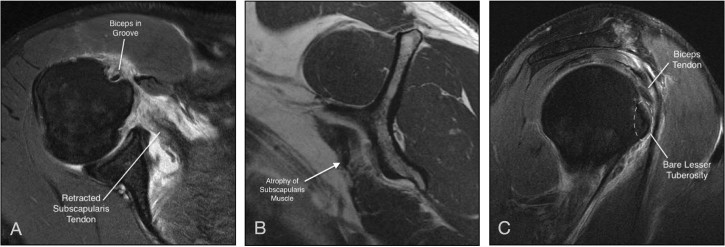
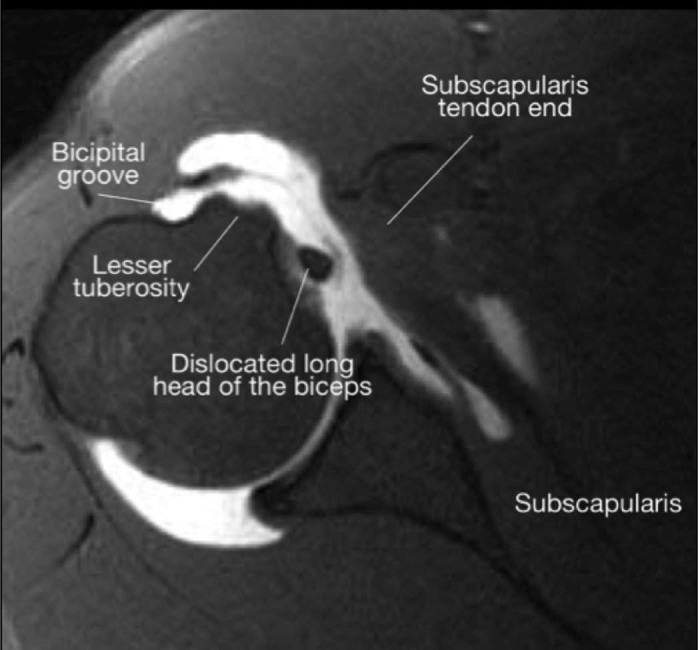
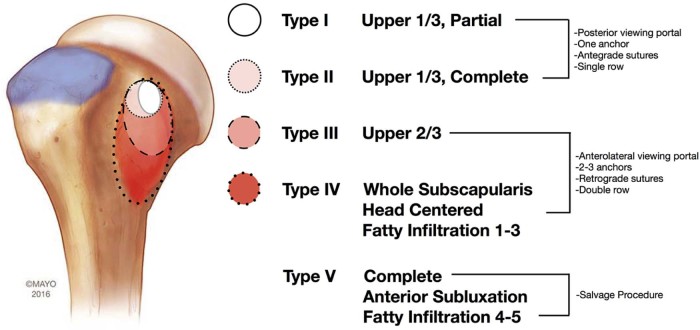
The subscapularis tendon, at one point, was thought of as the forgotten tendon, with "hidden lesions" that referred to partial tears of this tendon. Better understanding of anatomy and biomechanics combined with improved imaging technology and the widespread use of arthroscopy has led to a higher rate of subscapularis tear diagnoses and repairs. The bulk mass of the subscapularis muscle is more than that of all 3 other rotator cuff muscles combined. It functions as the internal rotator of the shoulder as the stout, rolled border of its tendon inserts onto the superior portion of the lesser tuberosity. A thorough history combined with specific physical examination maneuvers (including the bear hug, lift-off, and belly-press tests) is critical for accurate diagnosis. A systematic approach to advanced shoulder imaging also improves diagnostic capacity. Once identified, most subscapularis tendon tears can be successfully repaired arthroscopically. The Lafosse classification is useful as part of a treatment algorithm. Type I and II tears may be addressed while viewing from the standard posterior glenohumeral portal; larger Lafosse type III and IV tears are best repaired with anterior visualization at the subacromial or subdeltoid space. Tendon mobilization for larger tears is critical for adequate repair. In Lafosse type V tears, in which there is glenohumeral imbalance, tendon transfers and reverse replacement are commonly considered salvage options.
肩胛下肌腱曾一度被视为被遗忘的肌腱,存在“隐匿性损伤”,即该肌腱的部分撕裂。对解剖学和生物力学的深入理解,结合改进的成像技术以及关节镜的广泛应用,使得肩胛下肌撕裂的诊断和修复率有所提高。肩胛下肌的体积比其他三块肩袖肌肉的总和还要大。它作为肩部的内旋肌发挥作用,其肌腱厚实、卷曲的边缘插入小结节的上部。详细的病史结合特定的体格检查手法(包括熊抱试验、抬离试验和腹部按压试验)对于准确诊断至关重要。采用系统的方法进行肩部高级成像也能提高诊断能力。一旦确诊,大多数肩胛下肌腱撕裂可以通过关节镜成功修复。拉福斯分类法作为治疗方案的一部分很有用。I型和II型撕裂可通过标准的后盂肱关节入路进行处理;较大的拉福斯III型和IV型撕裂最好在前入路观察下于肩峰下或三角肌下间隙进行修复。对于较大的撕裂,肌腱的游离对于充分修复至关重要。在拉福斯V型撕裂中,即存在盂肱关节失衡的情况下,肌腱转移和反置置换通常被视为挽救性选择。