Chronic Disease Research Group, Hennepin Healthcare Research Institute, Minneapolis, Minnesota;
Department of Medicine, University of Minnesota, Minneapolis, Minnesota.
J Am Soc Nephrol. 2019 Feb;30(2):346-353. doi: 10.1681/ASN.2018060581. Epub 2019 Jan 24.
Morbidity and mortality vary seasonally. Timing and severity of influenza seasons contribute to those patterns, especially among vulnerable populations such as patients with ESRD. However, the extent to which influenza-like illness (ILI), a syndrome comprising a range of potentially serious respiratory tract infections, contributes to mortality in patients with ESRD has not been quantified.
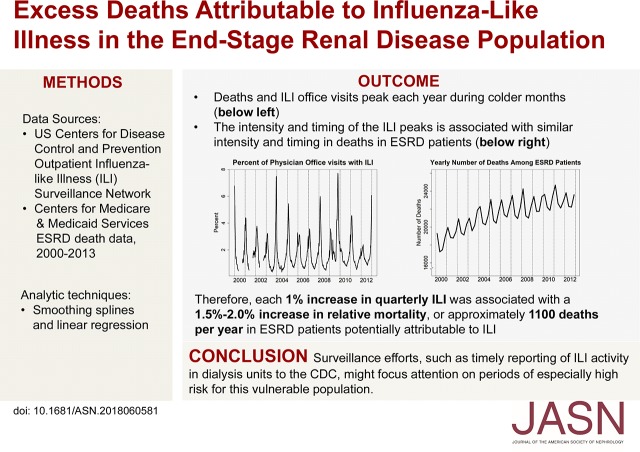
We used data from the Centers for Disease Control and Prevention (CDC) Outpatient Influenza-like Illness Surveillance Network and Centers for Medicare and Medicaid Services ESRD death data from 2000 to 2013. After addressing the increasing trend in deaths due to the growing prevalent ESRD population, we calculated quarterly relative mortality compared with average third-quarter (summer) death counts. We used linear regression models to assess the relationship between ILI data and mortality, separately for quarters 4 and 1 for each influenza season, and model parameter estimates to predict seasonal mortality counts and calculate excess ILI-associated deaths.
An estimated 1% absolute increase in quarterly ILI was associated with a 1.5% increase in relative mortality for quarter 4 and a 2.0% increase for quarter 1. The average number of annual deaths potentially attributable to ILI was substantial, about 1100 deaths per year.
We found an association between community ILI activity and seasonal variation in all-cause mortality in patients with ESRD, with ILI likely contributing to >1000 deaths annually. Surveillance efforts, such as timely reporting to the CDC of ILI activity within dialysis units during influenza season, may help focus attention on high-risk periods for this vulnerable population.
发病率和死亡率呈季节性变化。流感季节的时间和严重程度导致了这些模式,特别是在易受感染的人群中,如终末期肾病患者。然而,流感样疾病(ILI)的严重程度,即一系列潜在严重呼吸道感染的综合征,在多大程度上导致终末期肾病患者的死亡尚未被量化。
我们使用了疾病控制和预防中心(CDC)门诊流感样疾病监测网络和医疗保险和医疗补助服务中心 2000 年至 2013 年的终末期肾病死亡数据。在解决了由于不断增加的终末期肾病患者人群而导致的死亡人数增加的趋势之后,我们计算了与第三季度(夏季)平均死亡人数相比的季度相对死亡率。我们使用线性回归模型来评估 ILI 数据与死亡率之间的关系,分别为每个流感季节的第 4 季度和第 1 季度,并使用模型参数估计来预测季节性死亡人数并计算与 ILI 相关的超额死亡人数。
估计 ILI 每季度增加 1%,第 4 季度的相对死亡率增加 1.5%,第 1 季度增加 2.0%。每年可能归因于 ILI 的年死亡人数相当多,约为 1100 人。
我们发现社区 ILI 活动与终末期肾病患者全因死亡率的季节性变化之间存在关联,ILI 可能导致每年超过 1000 人死亡。监测工作,如在流感季节及时向 CDC 报告透析单位内的 ILI 活动,可能有助于关注这个脆弱人群的高危时期。