Rungjirajittranon Tarinee, Owattanapanich Weerapat
Division of Medicine, Phranangklao Hospital, Nonthaburi, Thailand.
Division of Hematology, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand.
J Med Case Rep. 2019 Jan 28;13(1):25. doi: 10.1186/s13256-018-1955-x.
Immune thrombocytopenia is an acquired autoimmune disease. Recently, there has been evidence of thrombotic risk in patients with immune thrombocytopenia, but the mechanism is still inconclusive. Intravenous immunoglobulin infusion therapy is considered an efficient treatment; however, it still is associated with adverse events of fever, chills, and hypotension, as well as serious complications such as thrombosis. We report a case a patient with relapsed immune thrombocytopenia who developed ischemic stroke after an intravenous immunoglobulin infusion.
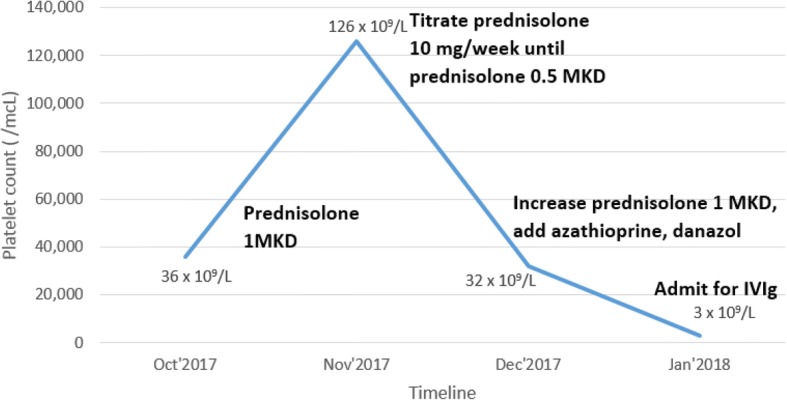
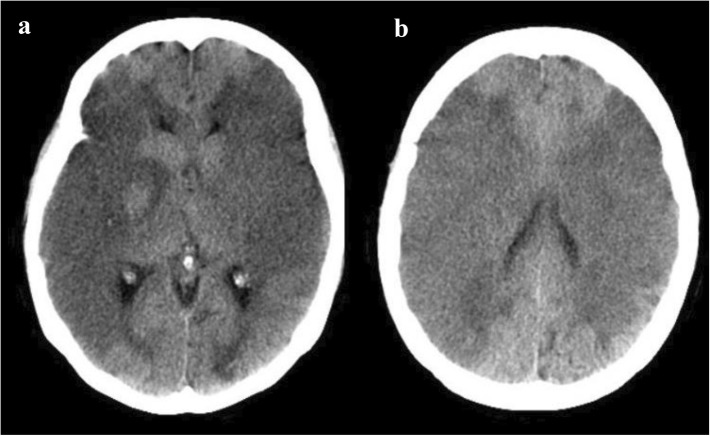
A 49-year-old Thai woman with relapsed/refractory immune thrombocytopenia came to our hospital with a large hematoma at the right buttock, and her platelet was decreased to 3 × 10/L. She was admitted to our hospital for intravenous immunoglobulin administration. One hour after completion of intravenous immunoglobulin infusion, the patient's sister complained that the patient was unconscious and could not move both legs and arms. Emergency computed tomography of the brain showed no abnormal findings, such as brain edema, intracranial hemorrhage, or infarction. One day later, repeat computed tomography of the brain displayed extensive acute ischemic changes and loss of gray-white differentiation of bilateral cerebral hemispheres.
We performed an extensive literature review to determine the possible causes of serious thrombotic events in immune thrombocytopenia between the predictive factors of the disease and intravenous immunoglobulin. Although intravenous immunoglobulin is an effective treatment, thrombotic complications can occur. We emphasize that in patients with atherosclerosis risk factors or thrombophilia, the appropriateness of administering an intravenous immunoglobulin infusion should be carefully evaluated.
免疫性血小板减少症是一种获得性自身免疫性疾病。最近,有证据表明免疫性血小板减少症患者存在血栓形成风险,但其机制仍无定论。静脉输注免疫球蛋白治疗被认为是一种有效的治疗方法;然而,它仍与发热、寒战和低血压等不良事件以及血栓形成等严重并发症相关。我们报告一例复发性免疫性血小板减少症患者在静脉输注免疫球蛋白后发生缺血性卒中的病例。
一名49岁的泰国女性,患有复发性/难治性免疫性血小板减少症,因右臀部出现巨大血肿前来我院就诊,其血小板计数降至3×10/L。她因静脉输注免疫球蛋白而入住我院。静脉输注免疫球蛋白结束1小时后,患者的妹妹称患者意识不清,双下肢和双臂均不能活动。脑部急诊计算机断层扫描未发现异常表现,如脑水肿、颅内出血或梗死。一天后,脑部重复计算机断层扫描显示双侧大脑半球广泛急性缺血改变及灰白质分界消失。
我们进行了广泛的文献综述,以确定免疫性血小板减少症中严重血栓事件的可能原因,该疾病的预测因素与静脉输注免疫球蛋白之间的关系。尽管静脉输注免疫球蛋白是一种有效的治疗方法,但仍可能发生血栓并发症。我们强调,对于有动脉粥样硬化危险因素或易栓症的患者,应仔细评估静脉输注免疫球蛋白的适宜性。