Brigham and Women's Hospital, Harvard Medical School, Boston, Massachusetts.
University of Massachusetts Medical School, Worcester.
Arthritis Rheumatol. 2019 May;71(5):712-721. doi: 10.1002/art.40834. Epub 2019 Apr 2.
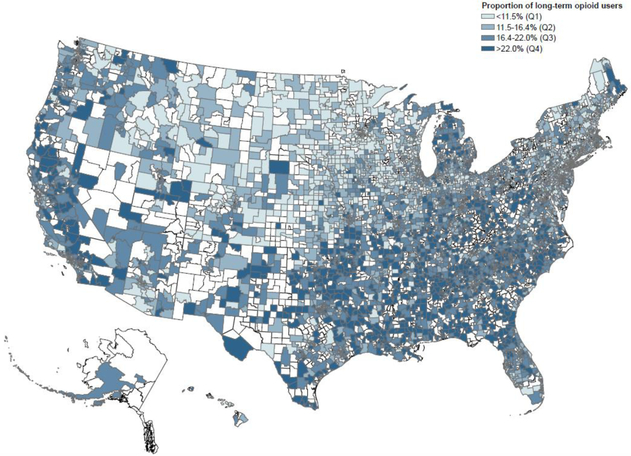
To evaluate the variation in long-term opioid use in osteoarthritis (OA) patients according to geography and health care access.
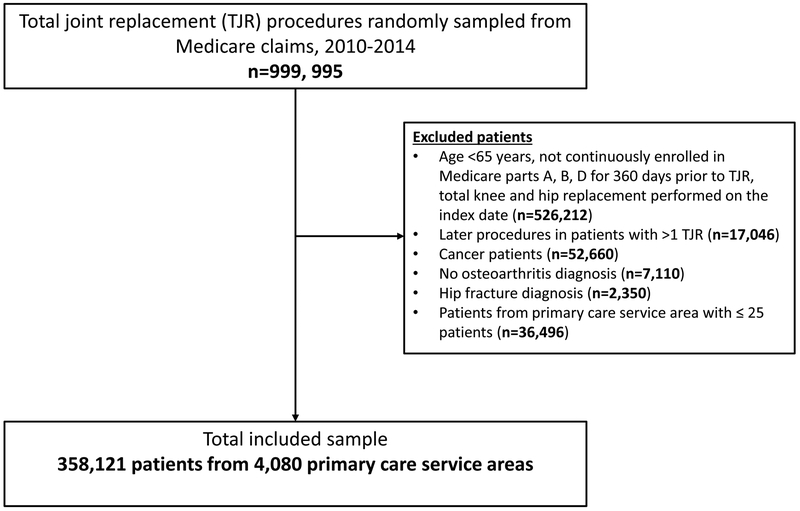
We designed an observational cohort study among OA patients undergoing total joint replacement (TJR) in the Medicare program (2010 through 2014). The independent variables of interest were the state of residence and health care access, which was quantified at the primary care service area (PCSA) level as categories of number of practicing primary care providers (PCPs) and categories of rheumatologists per 1,000 Medicare beneficiaries. The percentage of OA patients taking long-term opioids (≥90 days in the 360-day period immediately preceding TJR) within each PCSA was the outcome variable in a multilevel, generalized linear regression model, adjusting for case-mix at the PCSA level and for policies, including rigor of prescription drug monitoring programs and legalized medical marijuana, at the state level.
A total of 358,121 patients with advanced OA, with a mean age of 74 years, were included from 4,080 PCSAs. The unadjusted mean percentage of long-term opioid users varied widely across states, ranging from 8.9% (Minnesota) to 26.4% (Alabama), and this variation persisted in the adjusted models. Access to PCPs was only modestly associated with rates of long-term opioid use between PCSAs with highest (>8.6) versus lowest (<3.6) concentration of PCPs (adjusted mean difference 1.4% [95% confidence interval 0.8%, 2.0%]), while access to rheumatologists was not associated with long-term opioid use.
We note a substantial statewide variation in rates of long-term treatment with opioids in OA, which is not fully explained by the differences in access to health care providers, varying case-mix, or state-level policies.
根据地理位置和医疗保健可及性评估骨关节炎(OA)患者长期使用阿片类药物的情况。
我们设计了一项观察性队列研究,纳入了医疗保险计划(2010 年至 2014 年)中接受全关节置换术(TJR)的 OA 患者。感兴趣的自变量为居住州和医疗保健可及性,这是通过初级保健服务区域(PCSA)水平来量化的,具体为执业初级保健提供者(PCP)数量的类别和每 1000 名医疗保险受益人的风湿病医生数量的类别。每个 PCSA 中接受长期阿片类药物治疗(TJR 前 360 天内≥90 天)的 OA 患者的百分比是多水平、广义线性回归模型的因变量,该模型在 PCSA 水平上调整病例组合,并在州水平上调整政策,包括处方药物监测计划的严格程度和医用大麻合法化。
共纳入了 358121 名患有晚期 OA 的患者,平均年龄为 74 岁,来自 4080 个 PCSA。未经调整的长期阿片类药物使用者的百分比在各州之间差异很大,范围从 8.9%(明尼苏达州)到 26.4%(阿拉巴马州),在调整后的模型中这种差异仍然存在。与 PCSA 之间 PCP 浓度最高(>8.6)与最低(<3.6)相比,PCP 可及性仅与长期阿片类药物使用率之间存在适度关联(调整后的平均差异为 1.4%[95%置信区间为 0.8%,2.0%]),而风湿病医生的可及性与长期阿片类药物使用无关。
我们注意到 OA 长期接受阿片类药物治疗的全州范围内存在显著差异,这不能完全用医疗保健提供者可及性、不同的病例组合或州一级政策的差异来解释。