Mannschreck Diana B, Rubinfeld Roy S, Soiberman Uri S, Jun Albert S
The Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Georgetown University Medical Center & Washington Hospital Center, Washington, DC, United States.
Am J Ophthalmol Case Rep. 2019 Jan 9;13:140-142. doi: 10.1016/j.ajoc.2019.01.004. eCollection 2019 Mar.
To report diffuse lamellar keratitis (DLK) occurring in an eye that underwent epithelium-off (epi-off) corneal cross-linking (CXL) as a treatment for post-surgical ectasia and the successful treatment of progressive ectasia with a novel epi-on CXL and conductive keratoplasty (CK) treatment.
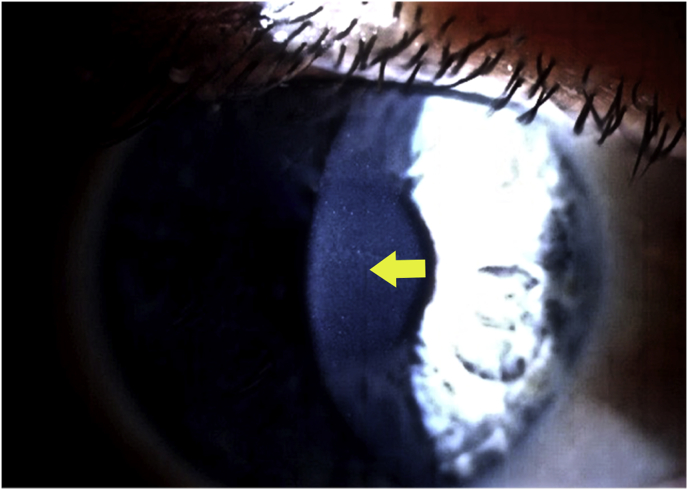
A 42-year-old man presented with corneal ectasia in his right eye 3 years after laser in situ keratomileusis (LASIK) surgery. He underwent epi-off corneal CXL using the Dresden protocol. Grade II DLK was diagnosed within days of CXL. Despite successful treatment of DLK, best-corrected visual acuity in the right eye deteriorated over the next 4 months due to progression of ectasia and remained worse than the patient's pre-operative baseline 1 year after epi-off CXL. Because of apparent disease progression, despite his CXL treatment, the patient underwent a novel, transepithelial CXL (TE-CXL) treatment combined with conductive keratoplasty (CK). This treatment improved his vision and stabilized his ectasia without subsequent DLK. Approximately 3 years after CK and TE-CXL, his eye remains stable with 4 Snellen lines of improved vision and no progression of ectasia.
Epithelium-off CXL is used increasingly to treat post-LASIK ectasia. First, in this case, DLK occurred after epi-off CXL. We suggest careful scrutiny of such cases as DLK is difficult to identify after epi-off CXL. Second, the epi-off CXL was unsuccessful in stopping the post-LASIK ectasia. Transepithelial CXL successfully treated the ongoing ectasia after resolution of the DLK with no subsequent re-occurrence of DLK. We suggest that TE-CXL may provide a successful initial treatment for post-LASIK ectasia that also minimizes the epithelial disruption that can lead to DLK.
报告一例接受上皮移除(epi-off)角膜交联术(CXL)治疗术后角膜扩张的患者发生弥漫性板层角膜炎(DLK),以及采用新型上皮在位(epi-on)CXL和传导性角膜成形术(CK)成功治疗进行性角膜扩张的情况。
一名42岁男性在准分子原位角膜磨镶术(LASIK)手术后3年出现右眼角膜扩张。他接受了采用德累斯顿方案的epi-off角膜CXL。在CXL术后数天内被诊断为Ⅱ级DLK。尽管DLK得到成功治疗,但右眼最佳矫正视力在接下来的4个月中因角膜扩张进展而恶化,在epi-off CXL术后1年仍低于患者术前基线水平。由于尽管进行了CXL治疗但疾病仍明显进展,该患者接受了新型的经上皮CXL(TE-CXL)治疗并联合传导性角膜成形术(CK)。这种治疗改善了他的视力并稳定了角膜扩张,且未再发生DLK。在CK和TE-CXL术后约3年,他的眼睛保持稳定,视力提高了4行Snellen视力表视力,且角膜扩张未进展。
Epithelium-off CXL越来越多地用于治疗LASIK术后角膜扩张。首先,在本病例中,epi-off CXL后发生了DLK。我们建议对此类病例进行仔细检查,因为epi-off CXL后DLK难以识别。其次,epi-off CXL未能成功阻止LASIK术后角膜扩张。经上皮CXL在DLK消退后成功治疗了持续的角膜扩张,且未再发生DLK。我们认为TE-CXL可能为LASIK术后角膜扩张提供一种成功的初始治疗方法,同时也最大限度地减少了可能导致DLK的上皮破坏。