Zdziarski Przemyslaw, Gamian Andrzej
Department of Immunology of Infectious Diseases, Ludwik Hirszfeld Institute of Immunology and Experimental Therapy, Polish Academy of Sciences, Wrocław, Poland.
Department of Clinical Immunology, Lower Silesian Center, Wrocław, Poland.
Front Pharmacol. 2019 Jan 18;9:1559. doi: 10.3389/fphar.2018.01559. eCollection 2018.
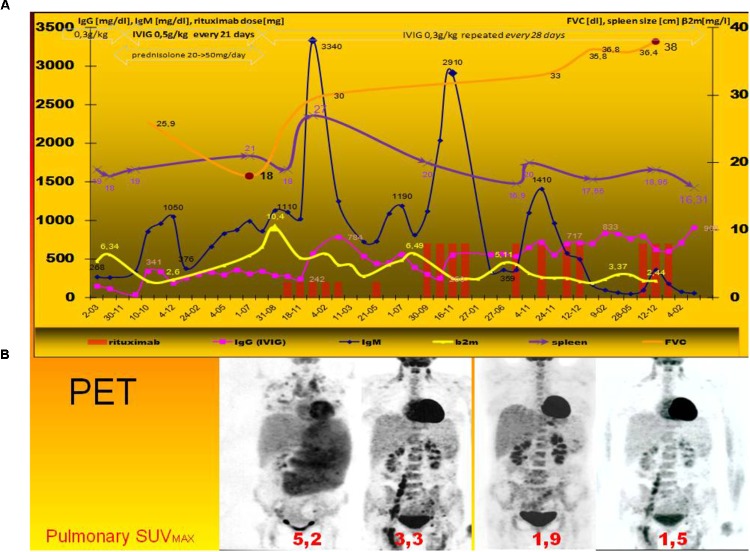
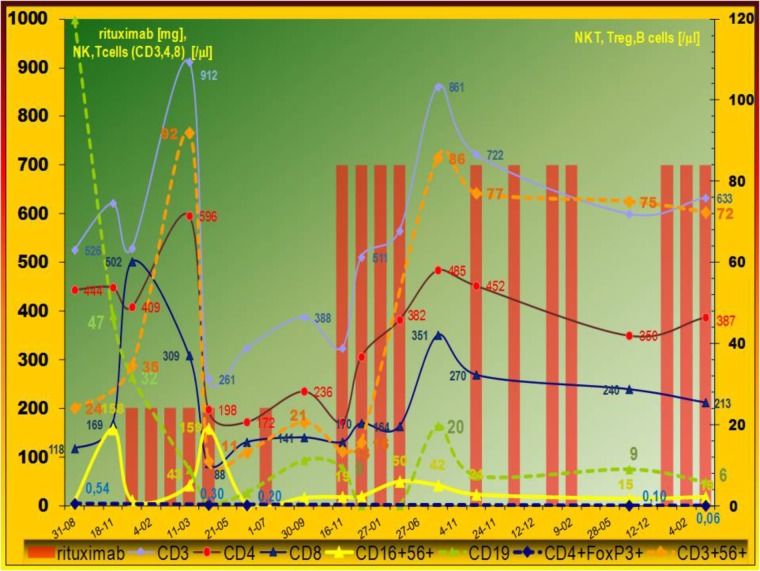
Lymphoid interstitial pneumonia (LIP) is a rare lymphoproliferative disease. LIP in common variable immunodeficiency (CVID) was observed in a patient during immunomodulatory therapy after progression of the disease (i.e., glucocorticoids, immunoglobulin dose escalation, and finally rituximab). Due to humoral immunodeficiency and serious serum sickness rituximab was used initially at a low dose (150 mg/m weekly). It resulted in temporary remission with the decrease of serum paraproteinemia, β-microglobulin (β2M) and SUV decrease as well as increase of FVC. Owing to the relapse after 6-month remission in the second cycle a standard dose of rituximab was used (375 mg/m). Therapeutic regimen with 375 mg/m of Rtx in optimal schedule (i.e., every 3 weeks) resulted in no longer remission but higher incidence of opportunistic infections. Finally, after another cycle of immunotherapy FVC, paraproteinemia and β2M level normalization were observed as well as the decrease of severe splenomegaly. In laboratory and immunological progress the increase of NK and NKT cells was observed after the initial dose but the standard one caused NK cell increase only. Unfortunately, the decrease of CD19+Bcells was comparable between both doses, as was the decline of FoxP3+ regulatory T cell. On the contrary, after the low dose absolute T cell (both CD4 and CD8) number decreased but after the standard one - it normalized. Rtx (especially in low dose) brought further increase of persistent T cell activation (CD38+ T cells made up 79%). Innate immune response and the decrease of Treg are a compensatory pathways for the decrease of B and T cells. Immunodeficiency requires a different investigative approach to a immunotherapy. ClinicalTrials.gov, NCT02789397.
淋巴样间质性肺炎(LIP)是一种罕见的淋巴增殖性疾病。一名患有常见可变免疫缺陷(CVID)的患者在疾病进展后接受免疫调节治疗(即糖皮质激素、免疫球蛋白剂量递增,最后使用利妥昔单抗)期间出现了LIP。由于体液免疫缺陷和严重的血清病,最初以低剂量(150mg/m²每周)使用利妥昔单抗。这导致了暂时缓解,血清副蛋白血症、β-微球蛋白(β2M)降低,标准化摄取值(SUV)下降,同时用力肺活量(FVC)增加。由于在第二个周期6个月缓解后复发,使用了标准剂量的利妥昔单抗(375mg/m²)。以最佳方案(即每3周一次)使用375mg/m²利妥昔单抗的治疗方案并未导致再次缓解,反而机会性感染的发生率更高。最后,在另一轮免疫治疗后,观察到FVC、副蛋白血症和β2M水平恢复正常,严重脾肿大也有所减轻。在实验室和免疫学进展方面,初始剂量后观察到自然杀伤(NK)细胞和自然杀伤T(NKT)细胞增加,但标准剂量仅导致NK细胞增加。不幸的是,两种剂量下CD19+B细胞的减少以及叉头框蛋白3(FoxP3)+调节性T细胞的下降相当。相反,低剂量后绝对T细胞(CD4和CD8)数量减少,但标准剂量后数量恢复正常。利妥昔单抗(尤其是低剂量)使持续的T细胞活化进一步增加(CD38+T细胞占79%)。固有免疫反应和调节性T细胞的减少是B细胞和T细胞减少的代偿途径。免疫缺陷需要对免疫治疗采取不同的研究方法。ClinicalTrials.gov,NCT02789397。