Di Benedetto Paolo, Beltrame Alessandro, Cicuto C, Battistella C, Gisonni Renato, Cainero Vanni, Causero Araldo
clinic of orthopaedics, University Hospital of Udine.
Acta Biomed. 2019 Jan 10;90(1-S):36-46. doi: 10.23750/abm.v90i1-S.8074.
It is recognised that a significant percetage of large and massive rotator cuff tears (RCT) cannot be anatomically repaired and this correlates with a worste outcome in terms of pain, active range of motion, increased incidence of retair. The aim of our work is to find reliable index on preoperative MRI shoulder image to assist orthopaedist in surgical planning of rotatator cuff tears repair.
We performed a retrospective study on a population on 131 patients undergoing arthroscopic cuff repair by a single expert surgeon. Pre-operative MRI images were evaluated by a single orthopaedist, trained on MRI shoulder images ad blinded to surgical outcome. For each magnetic resonance we evaluated the following 9 parameters: fatty Infiltration (FI), Patte Stage (PS), tear size measured in medial-lateral (ML) and anterior- posterior (AP) dimension, Tangent Sign (TS), Occupation Grade (OG), Acromion-Humeral Distance (AHD), Inferior Gleno-Humeral Distance (IGHD), Glenoid Version Angle (GVA). We divided population into two groups: patients who obtained a complete repair of RCT (n=110) and patients who obtained only a partial repair of RCT (n=21). For each MRI index we conducted statistical analysis (Student's t test, Mann- Whitney U test, Shapiro-Wilk test, Chi-square test, Fisher exact test, ROC curves and maximum Youden index) to find a Cut Off value useful to predict partial repair.
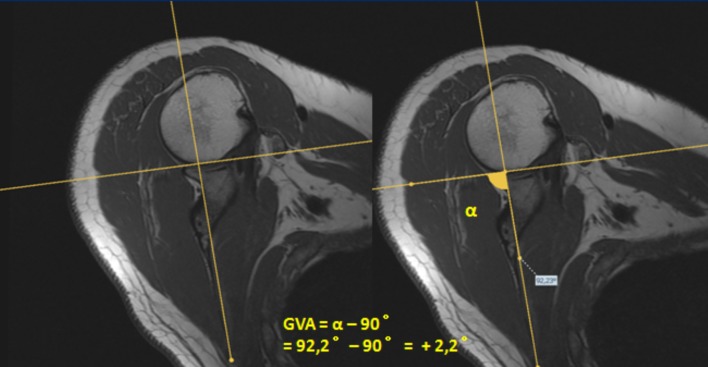
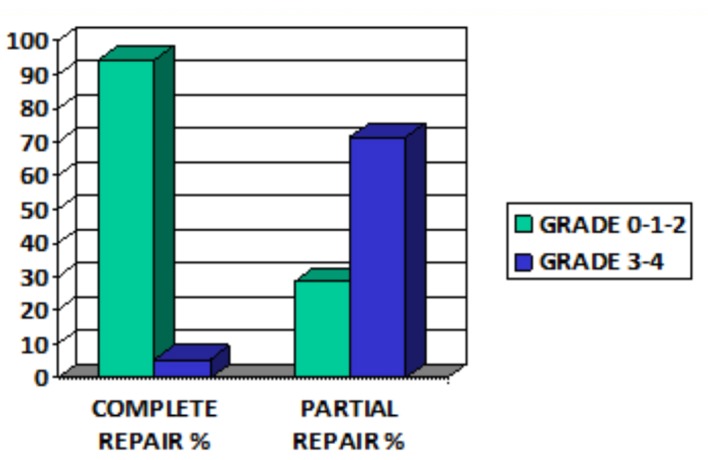
We have found statistical significance in predicting partial repair on MRI mesurements of Fatty Infiltration (FI grade ≥3; test di Fisher p<0.001), Patte Stage (grade= 3; test di Fisher p<0.001), Tear size measured in ML (>36 mm; Mann-Whitney p<0.001), Positive Tangent Sign (Chi-quadro p<0.001; sensitivity 95,3%, specificity 83,6%), Occupation Grade (OG <0,46; t-test p<0.001). Acromion-Humeral Distance (AHD <7 mm), Inferior Gleno-Humeral Distance (IGHD >5 mm). Tear size measured in AP (>21 mm; Mann-Whitney p<0.001) seems to be dependent on the contextual size of the lesion in ML. We haven't found statistical significance in predicting partial repair of Glenoid Version Angle.
A systematic observation of seven independent MRI parameters (FI, PS, tear size ML, TS, OG, AHD, IGHD) can help the surgeon to predict the impossibility to obtain complete repair of RCT and to consider different surgical approach.
人们认识到,相当一部分大型和巨大型肩袖撕裂(RCT)无法进行解剖修复,这与疼痛、主动活动范围、再撕裂发生率增加方面的更差结果相关。我们研究的目的是在术前肩部MRI图像上找到可靠指标,以协助骨科医生进行肩袖撕裂修复的手术规划。
我们对131例接受由同一位专家外科医生进行关节镜下肩袖修复的患者进行了回顾性研究。术前MRI图像由一位专门接受过肩部MRI图像培训且对手术结果不知情的骨科医生进行评估。对于每幅磁共振图像,我们评估了以下9个参数:脂肪浸润(FI)、帕特分期(PS)、在内侧-外侧(ML)和前后(AP)维度测量的撕裂大小、切线征(TS)、占据分级(OG)、肩峰-肱骨头距离(AHD)、下盂肱距离(IGHD)、盂肱关节面角(GVA)。我们将患者分为两组:RCT获得完全修复的患者(n = 110)和仅获得部分修复的患者(n = 21)。对于每个MRI指标,我们进行了统计分析(学生t检验、曼-惠特尼U检验、夏皮罗-威尔克检验、卡方检验、费舍尔精确检验、ROC曲线和最大约登指数),以找到有助于预测部分修复的临界值。
我们发现在预测部分修复方面,在MRI测量的脂肪浸润(FI分级≥3;费舍尔检验p < 0.001)、帕特分期(分级 = 3;费舍尔检验p < 0.001)、ML方向测量的撕裂大小(> 36 mm;曼-惠特尼检验p < 0.001)、阳性切线征(卡方检验p < 0.001;敏感性95.3%,特异性83.6%)、占据分级(OG < 0.46;t检验p < 0.001)、肩峰-肱骨头距离(AHD < 7 mm)、下盂肱距离(IGHD > 5 mm)方面存在统计学意义。AP方向测量的撕裂大小(> 21 mm;曼-惠特尼检验p < 0.001)似乎取决于ML方向病变的背景大小。我们未发现盂肱关节面角在预测部分修复方面有统计学意义。
对七个独立的MRI参数(FI、PS、撕裂大小ML、TS、OG、AHD、IGHD)进行系统观察,可帮助外科医生预测无法获得RCT完全修复的可能性,并考虑不同的手术方法。