Khan Muhammad Amir, Walley John D, Ali Saima, King Rebecca, Khan Shaheer Ellahi, Khan Nida, Sheikh Faisal Imtiaz, Khan Haroon Jehangir
Chief Coordinating Professional, Association for Social Development, Islamabad, Pakistan.
Professor of International Public Health, Nuffield Centre for International Health and Development, Leeds Institute of Health Sciences, University of Leeds, Leeds, UK.
BJGP Open. 2018 Nov 14;2(4):bjgpopen18X101612. doi: 10.3399/bjgpopen18X101612. eCollection 2018 Dec.
Integrated care for diabetes and associated conditions at primary level health facilities can make care available to a much larger population, especially in rural areas.
This process evaluation was to understand how the authors' integrated care was implemented and experienced by the care providers and patients, and to inform modifications prior to province-wide scale-up.
DESIGN & SETTING: The mixed-method study was conducted as part of a cluster randomised trial on integrated diabetes care at 14 public health facilities.
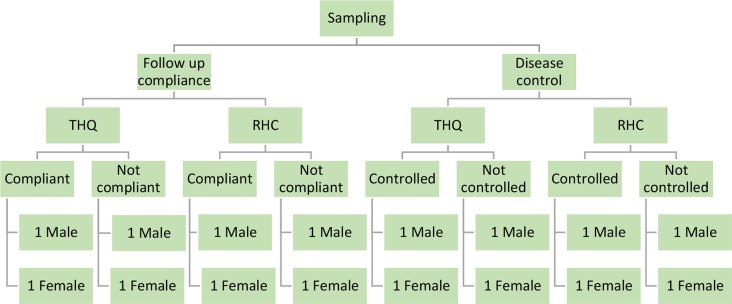
The care practices were assessed by analysing the routine clinical records of 495 registered patients with diabetes. Then semi-structured interviews with service providers and patients were used to understand their respective care experiences. A framework approach was applied to analyse and interpret the qualitative data.
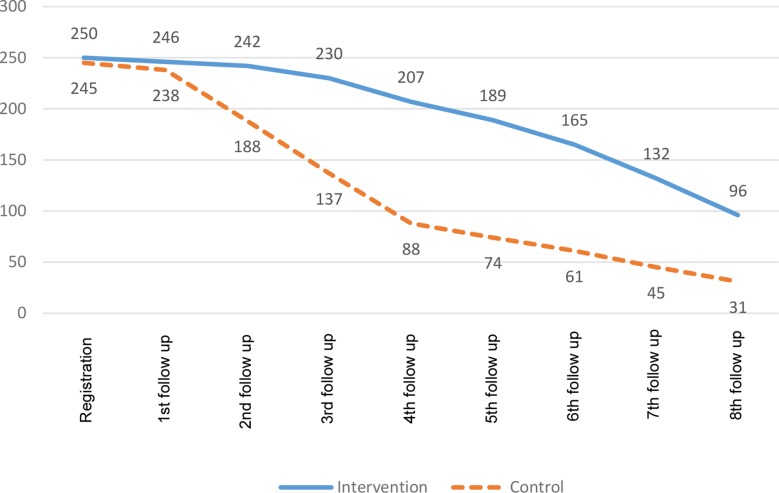
The intervention and the study were implemented as intended under routine conditions in rural health centres. Key service processes effectively delivered included: skill-based training; screening and diagnostic tests; treatment card records; and the additional case management as per desk guide, including monitoring progress in glucose and weight at follow-up consultations, and mobile phone calls to help adherence. However, social and cultural factors affected clients' ability to change lifestyles, especially for women. The intervention effect was limited by the short study follow-up of only 9 months.
Integrated diabetes care was feasible, both for providers and patients, and potentially scalable at primary care facilities under routine conditions in Pakistan. Additional operational interventions are required for sustained drug supplies, supervision, in-service training, and to address the social challenges to healthy activity and eating, especially for women.
基层医疗卫生机构对糖尿病及相关病症的综合护理能够让更多人获得医疗服务,尤其是在农村地区。
本过程评估旨在了解医护人员和患者如何实施及体验作者的综合护理,并为在全省范围内扩大规模之前进行调整提供依据。
这项混合方法研究是一项关于14家公共卫生机构糖尿病综合护理的整群随机试验的一部分。
通过分析495名登记糖尿病患者的常规临床记录来评估护理实践。然后,通过对服务提供者和患者进行半结构化访谈,了解他们各自的护理体验。采用框架法分析和解释定性数据。
在农村卫生中心的常规条件下,干预措施和研究按计划实施。有效提供的关键服务流程包括:基于技能的培训;筛查和诊断测试;治疗卡记录;以及根据案头指南进行的额外病例管理,包括在随访咨询时监测血糖和体重进展情况,以及通过手机通话促进依从性。然而,社会和文化因素影响了患者改变生活方式的能力,尤其是女性。干预效果因仅9个月的短期研究随访而受到限制。
在巴基斯坦的常规条件下,糖尿病综合护理对医护人员和患者而言都是可行的,并且在基层医疗设施中可能具有可扩展性。需要采取额外的运营干预措施来确保持续的药品供应、监督、在职培训,并应对健康活动和饮食方面的社会挑战,尤其是针对女性。