Hedsund Caroline, Ankjærgaard Kasper Linde, Rasmussen Daniel Bech, Schwaner Signe Høyer, Andreassen Helle Frost, Hansen Ejvind Frausing, Wilcke Jon Torgny
Department of Pulmonary Medicine, Gentofte Hospital, Hellerup, Denmark.
Respiratory Research Unit Zealand, Department of Respiratory Medicine, Naestved Hospital, Naestved, Denmark.
Eur Clin Respir J. 2019 Jan 29;6(1):1571332. doi: 10.1080/20018525.2019.1571332. eCollection 2019.
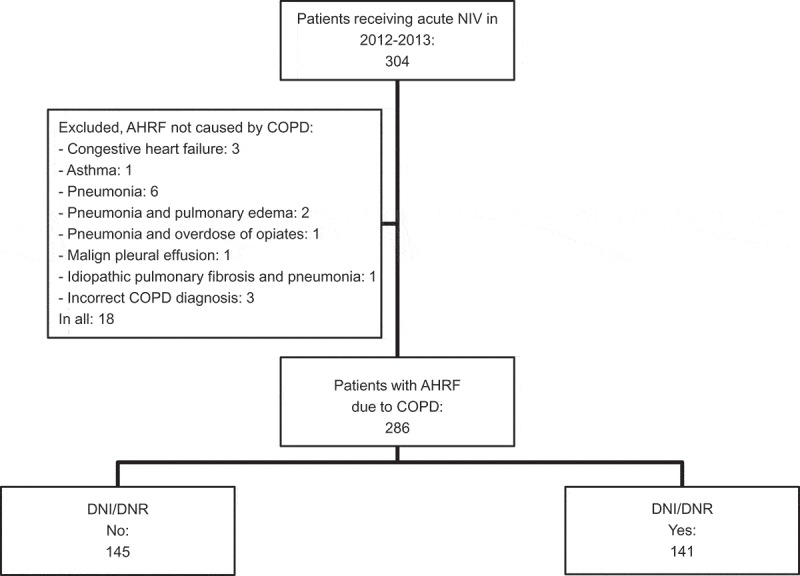
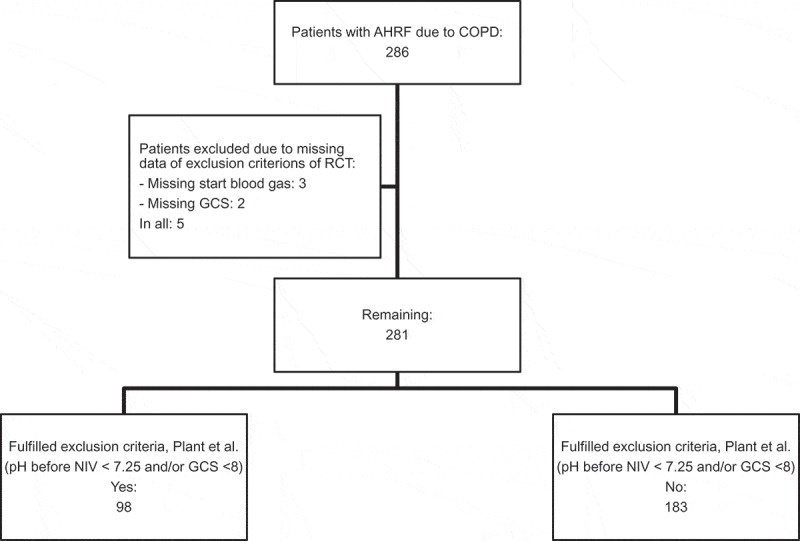
: Hospital mortality among chronic obstructive pulmonary disease (COPD) patients receiving NIV for acute respiratory failure has shown to be significantly higher in clinical settings than in the randomized trials (RCTs) which clinical guidelines are based on. This may be due to the quality of care of NIV or patient selection. In daily clinical practice, we include patients with terminal pulmonary disease with a do-not-intubate (DNI) or a do-not-resuscitate (DNR) order with a high mortality risk compared to highly selected patients in RCTs. The aim of this study was to determine the role of patient selection for in-hospital mortality among patients receiving NIV for acute respiratory failure of COPD. : We conducted a retrospective study including all patients receiving acute NIV due to acute respiratory failure at the respiratory wards in 2012-2013 at two hospitals in Greater Copenhagen. : Overall in-hospital mortality rate was 30%. In patients with a DNI/DNR order, mortality was 59% and in patients with no limitations in treatment 2%. Patients who fulfilled the exclusion criteria of the RCT by Plant et al. had a mortality of 41% compared to 25% in the remaining population. : High overall in-hospital mortality reflects that patient selection in clinical practice is very different from RCT. Quality of acute NIV treatment seems acceptable in clinical practice for patients with less severe COPD and no limitations in treatment. Higher mortality in patients with DNI/DNR order may be due to inefficient NIV treatment for these patients with more severe COPD.
在临床环境中,因急性呼吸衰竭接受无创通气(NIV)的慢性阻塞性肺疾病(COPD)患者的医院死亡率已显示出显著高于临床指南所基于的随机试验(RCT)中的死亡率。这可能归因于无创通气的护理质量或患者选择。在日常临床实践中,与随机试验中经过高度筛选的患者相比,我们纳入了患有晚期肺部疾病且有不要插管(DNI)或不要复苏(DNR)医嘱、死亡风险高的患者。本研究的目的是确定在因COPD急性呼吸衰竭接受无创通气的患者中,患者选择对院内死亡率的作用。
我们进行了一项回顾性研究,纳入了2012 - 2013年哥本哈根大区两家医院呼吸病房因急性呼吸衰竭接受急性无创通气的所有患者。
总体院内死亡率为30%。有DNI/DNR医嘱的患者死亡率为59%,治疗无限制的患者死亡率为2%。符合Plant等人随机试验排除标准的患者死亡率为41%,而其余患者的死亡率为25%。
较高的总体院内死亡率反映出临床实践中的患者选择与随机试验有很大不同。对于病情较轻且治疗无限制的COPD患者,急性无创通气治疗质量在临床实践中似乎是可以接受的。有DNI/DNR医嘱的患者死亡率较高可能是由于对这些病情更严重的COPD患者无创通气治疗效果不佳。