Focused Research Unit in Emergency Medicine, Hospital of Southern Denmark, Kresten Philipsens Vej 15, DK-6200, Aabenraa, Denmark.
Institute for Regional Health Research, University of Southern Denmark, JB Winsløw Vej 25, DK-5000, Odense, Denmark.
BMC Infect Dis. 2019 Feb 11;19(1):133. doi: 10.1186/s12879-019-3754-4.
Infectious gastroenteritis is common in the emergency department (ED). Patients infected with either Norovirus or toxigenic Clostridium difficile require special isolation procedures. The aims were to describe the aetiology of infectious gastroenteritis in the ED, evaluate whether current isolation procedures, based on clinical judgement are sufficient, and to identify information that might be used to identify patients requiring isolation.
Prospective, observational, multicentre study. We collected information on symptoms, vital signs, travel history, the recent use of antibiotics, and infectious contacts and tested faecal samples for Norovirus, C. difficile, and enteropathogenic bacteria.
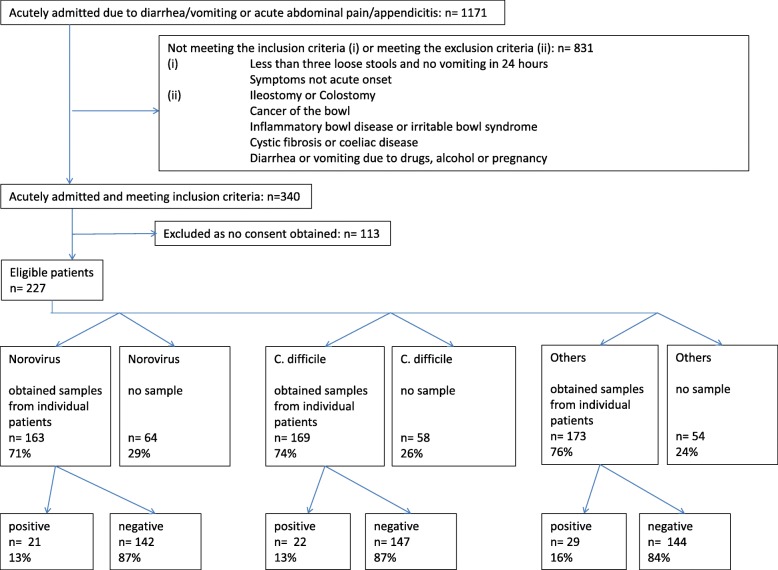
The study enrolled 227 patients, of whom 163 (71%) delivered a faecal sample for Norovirus analysis (13% positive), 171 (74%) for C. difficile (13% positive), and 173 (76%) for enteropathogenic bacteria (16% positive). In total 71% of the patients were isolated using strict precautions, 29% of the isolated patient and 14% of the patients who were not isolated had had a highly contagious GE. Risk factors for Norovirus included frequent vomiting (OR 5.5), recent admission of another patient with Norovirus (OR 2.6), and a short duration of diarrhoea. Risk factors for C. difficile infections included older age (OR 6.0), longer duration of diarrhoea (OR 5.2), mucus in stool (OR 3.5), and previous antibiotic use (OR 23.4).
Highly contagious GE occurs in ¼ of the GE patients in the EDs, isolation based on clinical judgement is not very efficient. Several risk factors can predict the presence of Norovirus or toxigenic Clostridium difficile. It is uncertain whether this knowledge can improve isolation practices in ED settings.
This study was retrospectively registered in the Clinical Trials Data Base ( NCT02685527 ) and prospectively approved by the Regional Committees on Health Research Ethics for Southern Denmark (project ID S20140200) and Ethics Committee at the Medical Association of Schleswig-Holstein ["Ethikkommission bei der Ärztekammer Schleswig-Holstein", project ID 120/15(I)] and registered with the Danish Data Protection Agency (project ID nr. 2008-58-0035/ 1608).
感染性胃肠炎在急诊科(ED)很常见。感染诺如病毒或产毒艰难梭菌的患者需要特殊的隔离程序。目的是描述 ED 中感染性胃肠炎的病因,评估基于临床判断的当前隔离程序是否足够,并确定可能用于识别需要隔离的患者的信息。
前瞻性、观察性、多中心研究。我们收集了症状、生命体征、旅行史、近期使用抗生素和感染接触的信息,并对粪便样本进行了诺如病毒、艰难梭菌和肠致病性细菌检测。
该研究共纳入 227 例患者,其中 163 例(71%)患者提供了粪便样本进行诺如病毒分析(13%阳性),171 例(74%)患者进行了艰难梭菌检测(13%阳性),173 例(76%)患者进行了肠致病性细菌检测(16%阳性)。共有 71%的患者采用严格的预防措施进行隔离,29%的隔离患者和 14%的未隔离患者患有高度传染性的 GE。诺如病毒感染的危险因素包括频繁呕吐(OR 5.5)、近期有另一名诺如病毒患者入院(OR 2.6)和腹泻持续时间短。艰难梭菌感染的危险因素包括年龄较大(OR 6.0)、腹泻持续时间较长(OR 5.2)、粪便中有粘液(OR 3.5)和近期使用抗生素(OR 23.4)。
高度传染性的 GE 在急诊科的 GE 患者中占四分之一,基于临床判断的隔离效率不高。一些危险因素可以预测诺如病毒或产毒艰难梭菌的存在。尚不确定这些知识是否能改善急诊科的隔离实践。
本研究在临床试验数据库中进行了回顾性注册(NCT02685527),并获得了南丹麦地区健康研究伦理委员会(项目 ID S20140200)和石勒苏益格-荷尔斯泰因州医学协会伦理委员会(项目 ID 120/15(I))的前瞻性批准,并向丹麦数据保护局(项目 ID nr. 2008-58-0035/1608)注册。