Epicentre, Paris, France.
Médecins Sans Frontières, Paris, France.
BMC Infect Dis. 2019 Feb 11;19(1):132. doi: 10.1186/s12879-019-3775-z.
Empirical treatment of tuberculosis (TB) may be necessary in patients with negative or no Xpert MTB/RIF results. In a context with access to Xpert, we assessed mortality in the 6 months after the initial TB consultation among HIV-positive and HIV-negative patients who received empirical TB treatment or TB treatment based on bacteriological confirmation and we compared it with the mortality among those who did not receive TB treatment.
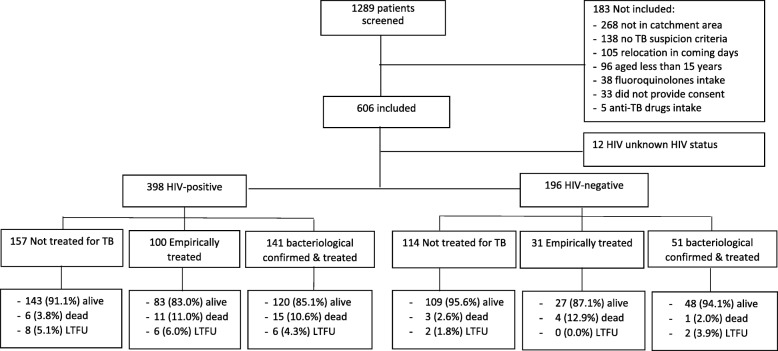
This prospective cohort study included consecutively adult patients with signs and symptoms of TB attending an outpatient TB clinic in Western Kenya. At the first consultation, patients received a clinical exam and chest X-ray. Sputum was collected for microscopy, Xpert and Mycobacterium tuberculosis complex (MTB) culture. Patients not started on TB treatment were reassessed after 5 days. All patients bacteriologically confirmed (positive Xpert or culture) received TB treatment. Empirical treatment was defined as a decision to start TB treatment without bacteriological confirmation. Patients were reassessed after 6 months.
Of 606 patients included, 344/606 (56.8%) were women. Median age was 35 years [Interquartile Range (IQR):27-47] and 398/594 (67.0%) were HIV-positive. In total, 196/606 (32.3%) patients were Xpert- or culture-positive and 331/606 (54.6%) started TB treatment. Overall, 100/398 (25.1%) HIV-positive and 31/196 (15.8%) HIV-negative patients received empirical treatment. Mortality in the 6 months following the first consultation was 1.6 and 0.8/100 patient-months among HIV-positive and HIV-negative patients respectively. In the multivariate analyses, TB treatment - whether empirical or based on bacteriological confirmation- was not associated with increased mortality among HIV-positive patients (aHR:2.51, 95%CI:0.79-7.90 and aHR:1.25, 95%CI:0.37-4.21 respectively). However, HIV-negative patients who received empirical treatment had a higher risk of mortality (aHR:4.85, 95%CI:1.08-21.67) compared to those not started on treatment. HIV-negative patients treated for TB based on bacteriological confirmation did not have a different risk of mortality (aHR:0.77, 95%CI:0.08-7.41).
Our findings suggest that in a context with access to Xpert, clinicians should continue using empirical TB treatment in HIV-positive patients with signs and symptoms of TB and negative Xpert results. However, differential diagnoses other than TB should be actively sought before initiating empirical TB treatment, particularly in HIV-negative patients.
对于 Xpert MTB/RIF 检测结果为阴性或无法检测的结核病(TB)患者,可能需要进行经验性治疗。在能够获得 Xpert 的情况下,我们评估了在首次 TB 就诊后 6 个月内,接受经验性 TB 治疗或基于细菌学确诊的 TB 治疗的 HIV 阳性和 HIV 阴性患者的死亡率,并与未接受 TB 治疗的患者的死亡率进行了比较。
这是一项前瞻性队列研究,纳入了肯尼亚西部一家门诊 TB 诊所出现 TB 症状和体征的连续成年患者。在首次就诊时,患者接受了临床检查和胸部 X 光检查。收集痰液进行显微镜检查、Xpert 和结核分枝杆菌复合群(MTB)培养。未开始 TB 治疗的患者在 5 天后重新评估。所有细菌学确诊(Xpert 阳性或培养阳性)的患者均接受 TB 治疗。经验性治疗是指在没有细菌学确诊的情况下决定开始 TB 治疗。患者在 6 个月后重新评估。
在 606 名患者中,344/606(56.8%)为女性。中位年龄为 35 岁[四分位间距(IQR):27-47],398/594(67.0%)为 HIV 阳性。共有 196/606(32.3%)患者 Xpert 或培养阳性,331/606(54.6%)开始 TB 治疗。总体而言,100/398(25.1%)名 HIV 阳性患者和 31/196(15.8%)名 HIV 阴性患者接受了经验性治疗。首次就诊后 6 个月的死亡率分别为 HIV 阳性患者 1.6/100 患者月和 HIV 阴性患者 0.8/100 患者月。在多变量分析中,无论经验性治疗还是基于细菌学确诊的 TB 治疗,均与 HIV 阳性患者的死亡率增加无关(调整后 HR:2.51,95%CI:0.79-7.90 和 aHR:1.25,95%CI:0.37-4.21)。然而,接受经验性治疗的 HIV 阴性患者的死亡率风险更高(aHR:4.85,95%CI:1.08-21.67),与未开始治疗的患者相比。基于细菌学确诊接受 TB 治疗的 HIV 阴性患者的死亡率没有差异(aHR:0.77,95%CI:0.08-7.41)。
我们的研究结果表明,在能够获得 Xpert 的情况下,对于出现 TB 症状和体征且 Xpert 结果为阴性的 HIV 阳性患者,临床医生应继续使用经验性 TB 治疗。然而,在开始经验性 TB 治疗之前,应积极寻找除 TB 以外的其他鉴别诊断,尤其是在 HIV 阴性患者中。