Martherus Tessa, Oberthuer André, Dekker Janneke, Kirchgaessner Christoph, van Geloven Nan, Hooper Stuart B, Kribs Angela, Te Pas Arjan B
Department of Paediatrics, Leiden University Medical Center, Leiden, Netherlands.
Department of Neonatology, Children's Hospital University of Cologne, Cologne, Germany.
Front Pediatr. 2019 Jan 29;7:3. doi: 10.3389/fped.2019.00003. eCollection 2019.
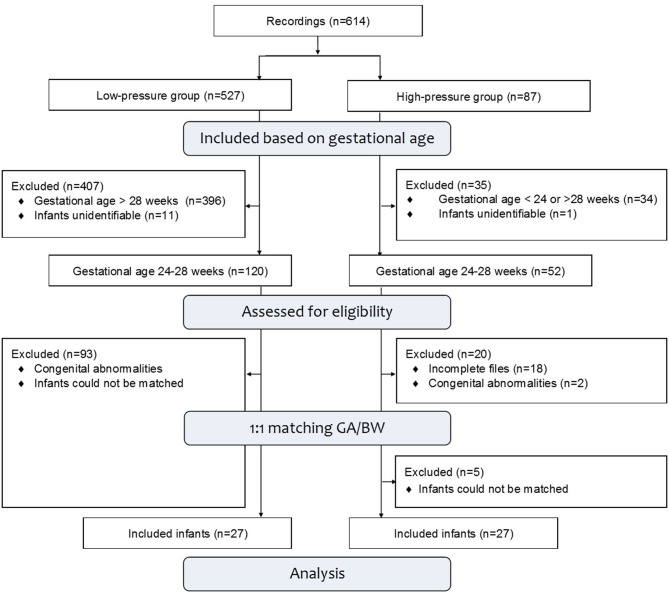
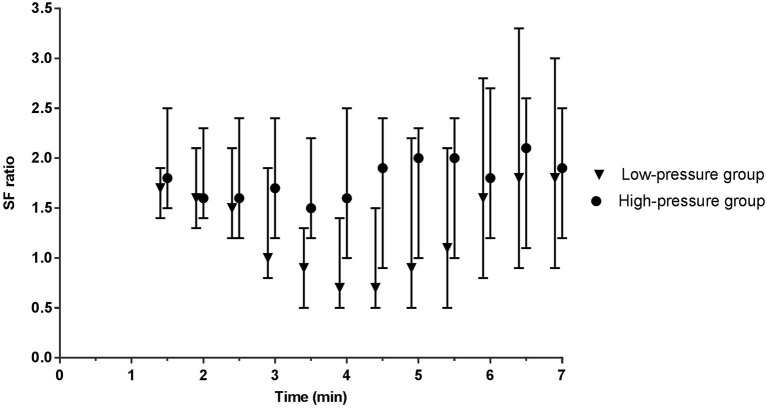
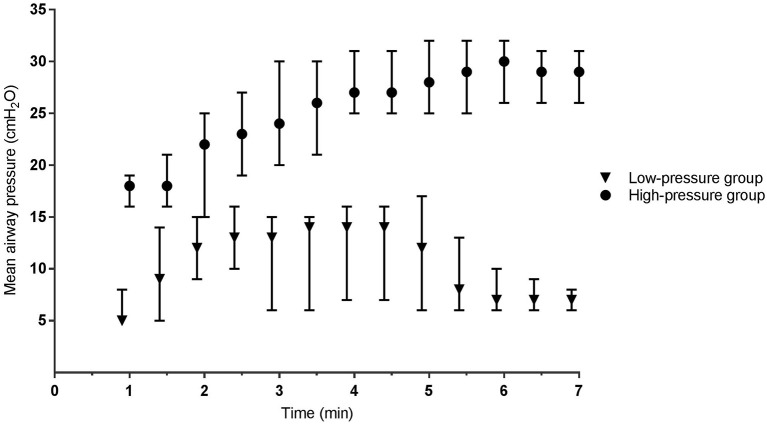
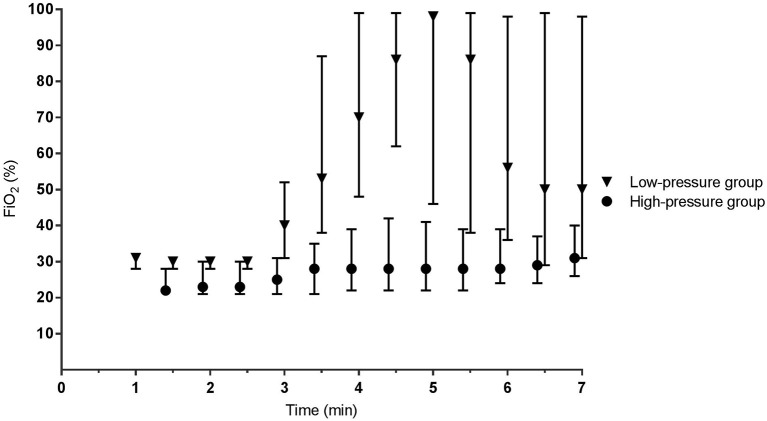
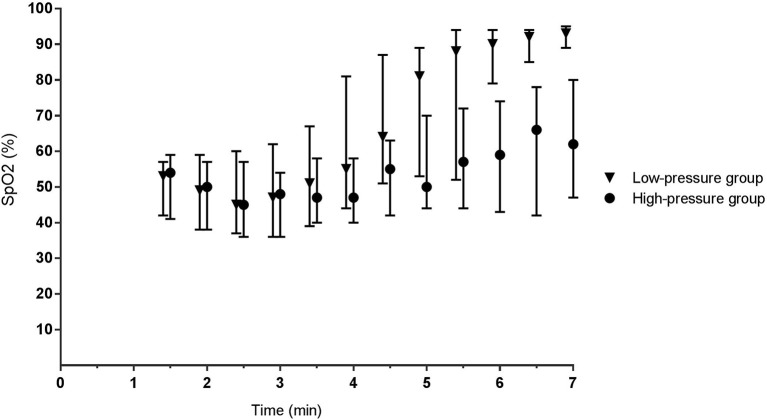
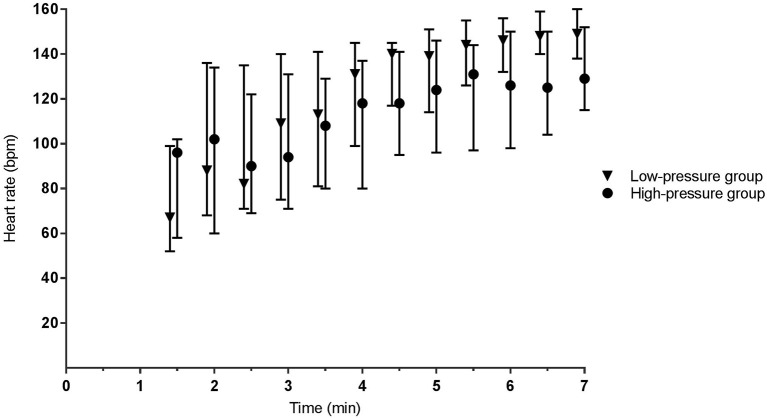
Respiratory support for stabilizing very preterm infants at birth varies between centers. We retrospectively compared two strategies that involved either increasing continuous positive airway pressures (CPAP), or increasing oxygen supplementation. Matched-pairs of infants (<28 weeks of gestation) were born either at the Leiden University Medical Center [low-pressure: CPAP 5-8 cmHO and/or positive pressure ventilation (PPV) and fraction of inspired oxygen (FiO) 0.3-1.0; = 27], or at the University Hospital of Cologne (high-pressure: CPAP 12-35 cmHO, no PPV and FiO 0.3-0.4; = 27). Respiratory support was initiated non-invasively via facemask at both units. Infants ( = 54) were matched between centers for gestational age and birth weight, to compare physiological and short-term clinical outcomes. In the low-pressure group, 20/27 (74%) infants received 1-2 sustained inflations (20, 25 cm HO) and 22/27 (81%) received PPV (1:19-3:01 min) using pressures of 25-27 cm HO. Within 3 min of birth [median (IQR)], mean airway pressures [12 (6-15) vs. 19 (16-23) cmHO, < 0.001] and FiO [0.30 (0.28-0.31) vs. 0.22 (0.21-0.30), < 0.001] were different in low- vs. high-pressure groups, respectively. SpO and heart rates were similar. After 3 min, higher FiO levels [0.62 (0.35-0.98) vs. 0.28 (0.22-0.38), = 0.005] produced higher SpO levels [77 (50-92) vs. 53 (42-69)%, < 0.001] in the low-pressure group, but SpO/FiO and heart rates were similar. While intubation rates during admission were significantly different (70 vs. 30%, = 0.013), pneumothorax rates (4 vs. 19%, = 0.125) and the occurrence of spontaneous intestinal perforations (0 vs. 15%, = 0.125) were similar between groups. Infants (<28 weeks) can be supported non-invasively at birth with either higher or lower pressures and while higher-pressure support may require less oxygen, it does not eliminate the need for oxygen supplementation. Future studies need to examine the effect of high pressures and pressure titration in the delivery room.
出生时用于稳定极早产儿的呼吸支持在不同中心有所不同。我们回顾性比较了两种策略,一种是增加持续气道正压(CPAP),另一种是增加氧气补充。对胎龄小于28周的婴儿进行配对,这些婴儿分别在莱顿大学医学中心出生(低压组:CPAP为5 - 8 cmH₂O和/或正压通气(PPV),吸入氧分数(FiO₂)为0.3 - 1.0;n = 27),或在科隆大学医院出生(高压组:CPAP为12 - 35 cmH₂O,无PPV,FiO₂为0.3 - 0.4;n = 27)。两个单位均通过面罩进行无创呼吸支持启动。在两个中心之间,根据胎龄和出生体重对54名婴儿进行配对,以比较生理和短期临床结局。在低压组中,27名婴儿中有20名(74%)接受了1 - 2次持续充气(20、25 cmH₂O),27名婴儿中有22名(81%)使用25 - 27 cmH₂O的压力接受了PPV(1:19 - 3:01分钟)。出生后3分钟内[中位数(四分位间距)],低压组与高压组的平均气道压力[12(6 - 15)vs. 19(16 - 23)cmH₂O,P < 0.001]和FiO₂[0.30(0.28 - 0.31)vs. 0.22(0.21 - 0.30),P < 0.001]分别不同。血氧饱和度(SpO₂)和心率相似。3分钟后,低压组中较高的FiO₂水平[0.62(0.35 - 0.98)vs. 0.28(0.22 - 0.38),P = 0.005]产生了较高的SpO₂水平[77(50 - 92)vs. 53(42 - 69)%,P < 0.001],但SpO₂/FiO₂和心率相似。虽然入院期间的插管率有显著差异(70% vs. 30%,P = 0.013),但两组间气胸发生率(4% vs. 19%,P = 0.125)和自发性肠穿孔发生率(0% vs. 15%,P = 0.125)相似。胎龄小于28周的婴儿出生时可以通过较高或较低压力进行无创支持,虽然高压支持可能需要较少的氧气,但并不能消除氧气补充的需求。未来的研究需要考察产房内高压和压力滴定的效果。