Sakai Yoshihito, Matsui Hiroki, Ito Sadayuki, Hida Tetsuro, Ito Kenyu, Koshimizu Hiroyuki, Harada Atsushi
Department of Orthopaedic Surgery, National Center for Geriatrics and Gerontology, Obu, Japan.
Department of Orthopaedic Surgery, Nagoya University School of Medicine, Nagoya, Japan.
Osteoporos Sarcopenia. 2017 Dec;3(4):195-200. doi: 10.1016/j.afos.2017.09.001. Epub 2017 Nov 13.
The prevalence of chronic low back pain (CLBP) increases with age and several mechanisms are involved in the development of CLBP, including osteoporosis; however, no associations with sarcopenia have yet been identified.
In total, 100 patients with CLBP and 560 patients without CLBP (nCLBP) aged over 65 years were studied. Skeletal muscle mass index (SMI) and percentage of body fat were evaluated using whole-body dual-energy X-ray absorptiometry. Sarcopenia was diagnosed when the relative SMI was more than 2 standard deviations below the mean in young adults. Thus, the cutoff value for sarcopenia was defined according to Sanada's Japanese population data. Paraspinal muscle cross-sectional areas of the lumbar multifidus and the erector spinae muscles were calculated using magnetic resonance imaging.
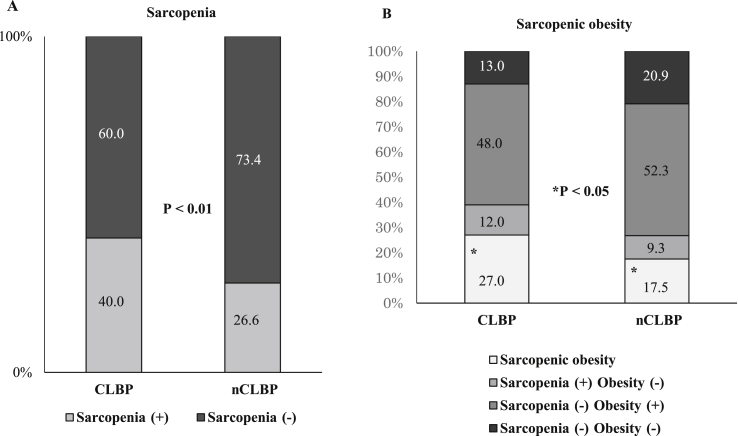
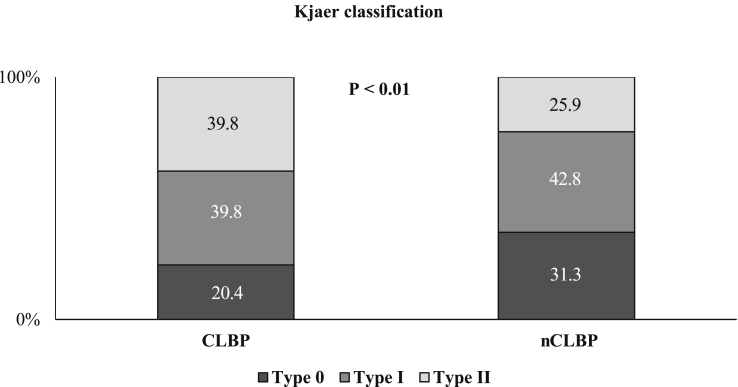
Forty patients (40.0%) from the CLBP group and 149 (26.6%) from the nCLBP group met the criteria of sarcopenia. SMI was significantly lower and the body fat ratio was significantly higher in the CLBP group compared with the nCLBP group. Sarcopenic obesity was significantly observed in the CLBP group. Lumbar multifidus and the erector spinae muscle cross sectional area were significantly lower in the CLBP group.
Elderly patients with CLBP have significantly lower skeletal muscle mass, and age-related mechanisms in sarcopenia are considered to be associated with chronic pain. Therapeutic procedures that are used to treat elderly aging muscle, including muscle strengthening and performance training, can possibly be a treatment for or used to prevent elderly CLBP.
慢性下腰痛(CLBP)的患病率随年龄增长而增加,其发病涉及多种机制,包括骨质疏松症;然而,尚未发现与肌肉减少症有关联。
共研究了100例65岁以上的CLBP患者和560例无CLBP(nCLBP)患者。采用全身双能X线吸收法评估骨骼肌质量指数(SMI)和体脂百分比。当相对SMI低于年轻人平均值2个标准差以上时,诊断为肌肉减少症。因此,根据Sanada的日本人群数据确定肌肉减少症的临界值。使用磁共振成像计算腰多裂肌和竖脊肌的椎旁肌横截面积。
CLBP组40例(40.0%)患者和nCLBP组149例(26.6%)患者符合肌肉减少症标准。与nCLBP组相比,CLBP组的SMI显著降低,体脂率显著升高。CLBP组中肌肉减少性肥胖显著。CLBP组的腰多裂肌和竖脊肌横截面积显著降低。
老年CLBP患者的骨骼肌质量显著降低,肌肉减少症的年龄相关机制被认为与慢性疼痛有关。用于治疗老年肌肉衰老的治疗方法,包括肌肉强化和功能训练,可能是治疗或预防老年CLBP的一种方法。