Brigham and Women's Hospital, Boston, Massachusetts.
Brigham and Women's Hospital and Harvard Medical School, Boston, Massachusetts.
Arthritis Care Res (Hoboken). 2019 Jul;71(7):914-924. doi: 10.1002/acr.23837.
To investigate the impact and timing of smoking cessation on developing rheumatoid arthritis (RA) and serologic phenotypes.
We investigated smoking cessation and RA risk in the Nurses' Health Study (NHS) (1976-2014) and the NHS II (1989-2015). Smoking exposures and covariates were obtained by biennial questionnaires. Self-reported RA was confirmed by medical record review for American College of Rheumatology/European League Against Rheumatism criteria. Cox regression was used to estimate hazard ratios (HRs) and 95% confidence intervals (95% CIs) for RA serologic phenotypes (all, seropositive, seronegative) according to smoking status, intensity, pack-years, and years since cessation.
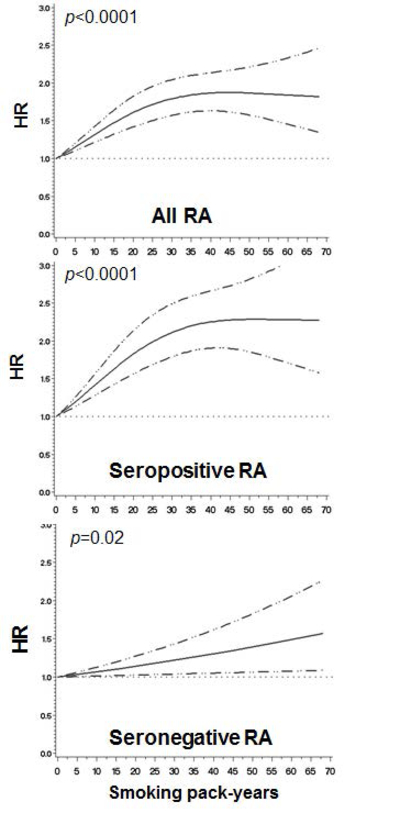
Among 230,732 women, we identified 1,528 incident cases of RA (63.4% of which were seropositive) during 6,037,151 person-years of follow-up. Compared with never smoking, current smoking increased the risk of all RA (multivariable HR 1.47, 95% CI 1.27-1.72) and seropositive RA (HR 1.67, 95% CI 1.38-2.01) but not seronegative RA (HR 1.20, 95% CI 0.93-1.55). An increasing number of smoking pack-years was associated with an increased trend for the risk of all RA (P < 0.0001) and seropositive RA (P < 0.0001). With increasing duration of smoking cessation, a decreased trend for the risk of all RA was observed (P = 0.009) and seropositive RA (P = 0.002). Compared to recent quitters (<5 years), those who quit ≥30 years ago had an HR of 0.63 (95% CI 0.44-0.90) for seropositive RA. However, a modestly increased risk of RA was still detectable 30 years after quitting smoking (for all RA, HR 1.25 [95% CI 1.02-1.53]; for seropositive RA, HR 1.30 [95% CI 1.01-1.68]; reference, never smoking).
These results confirm that smoking is a strong risk factor for developing seropositive RA and demonstrate for the first time that a behavior change of sustained smoking cessation could delay or even prevent seropositive RA.
研究戒烟对类风湿关节炎(RA)发病和血清学表型的影响及其发生时间。
我们对护士健康研究(NHS)(1976-2014 年)和 NHS II(1989-2015 年)中的戒烟与 RA 风险进行了研究。通过每两年一次的问卷获取吸烟暴露情况和协变量。根据美国风湿病学会/欧洲抗风湿病联盟标准,通过病历复查来确认自报的 RA。采用 Cox 回归估计 RA 血清学表型(所有、阳性、阴性)的风险比(HR)和 95%置信区间(95%CI),并根据吸烟状况、吸烟强度、吸烟包年数和戒烟年限进行分层。
在 230732 名女性中,我们在 6037151 人年的随访期间发现了 1528 例 RA 新发病例(其中 63.4%为阳性)。与从不吸烟相比,当前吸烟增加了所有 RA(多变量 HR 1.47,95%CI 1.27-1.72)和血清阳性 RA(HR 1.67,95%CI 1.38-2.01)的风险,但未增加血清阴性 RA(HR 1.20,95%CI 0.93-1.55)的风险。吸烟包年数的增加与所有 RA(P<0.0001)和血清阳性 RA(P<0.0001)风险呈增加趋势相关。随着戒烟时间的延长,所有 RA(P=0.009)和血清阳性 RA(P=0.002)的风险呈下降趋势。与近期戒烟者(<5 年)相比,戒烟≥30 年者血清阳性 RA 的 HR 为 0.63(95%CI 0.44-0.90)。然而,戒烟 30 年后仍能检测到 RA 风险略有增加(所有 RA,HR 1.25[95%CI 1.02-1.53];血清阳性 RA,HR 1.30[95%CI 1.01-1.68];参考值,从不吸烟)。
这些结果证实吸烟是发生血清阳性 RA 的一个强有力的危险因素,并首次表明持续戒烟这一行为改变可以延缓甚至预防血清阳性 RA 的发生。