Center for General Practice at Aalborg University, Fyrkildevej 7, 9220, Aalborg, Denmark.
Sansom Institute for Health Research, University of South Australia, GPO Box 2471, Adelaide, South Australia, 5001, Australia.
BMC Fam Pract. 2019 Feb 21;20(1):30. doi: 10.1186/s12875-019-0923-x.
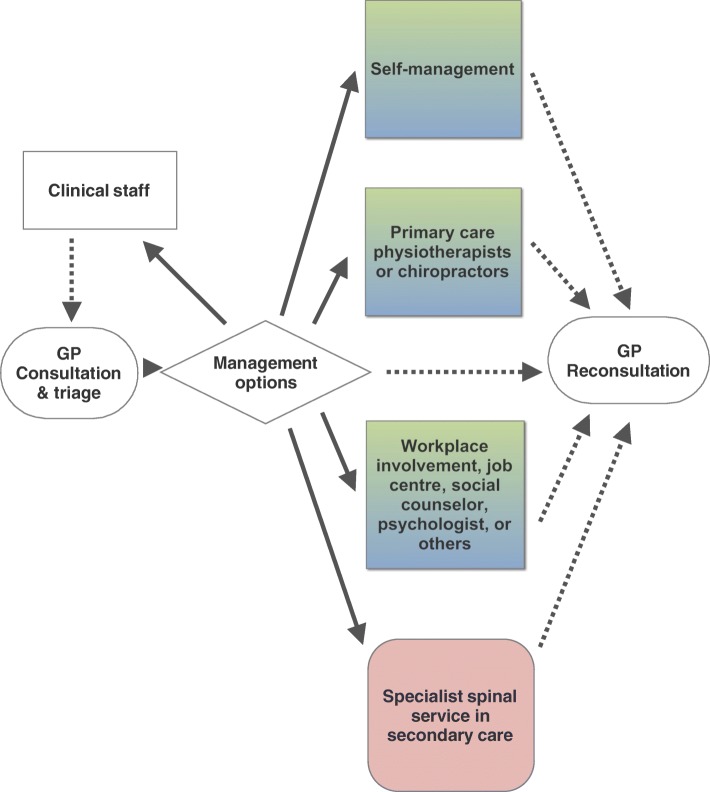
Low back pain affects about 80% of all adults, many of whom consult general practice. Providing management can be challenging, in part due to the scarcity of effective treatment methods. There is broad consensus in international clinical practice guidelines to provide patients with information about the nature of their pain and recommend them to stay active despite discomfort. Delivering this information is time-demanding and challenged by the limited available resources in general practice in many countries. Furthermore, general practice settings are highly variable in size and in their composition of clinical staff members - which presents difficulties, but also opportunities for developing alternative approaches to clinical management. Expanding the patient consultation time by involving clinical staff members (aside from the general practitioner) has been found feasible for other conditions. We propose that this approach is applied for non-specific low back pain. Consequently, we suggest the involvement of clinical staff members as part of a new strategy for managing low back pain in general practice.
Multifaceted implementation strategies have the potential to effectively enable change in the clinical management of patients with low back pain in general practice if they are based on theory and are tailored to stake holders. Inspired by the Medical Research Council's guidance for complex interventions and the ChiPP (Change in professional performance) statement, we suggest applying the following two policy categories: organizational change (environmental/social planning) and service provision. This will involve attention to environmental restructuring, modelling, enabling, education, training, persuasion, and incentivising of general practices, with an over-arching strategy of involving clinical staff members in the management of low back pain.
This is a pre-clinical proposal of a multifaceted strategy to support the delivery of evidence-based treatment for patients with low back pain in general practice. As an original idea, we suggest it would be feasible to involve clinical staff members in the delivery of information and advice to patients, whilst the general practitioner remains responsible for diagnostic decision-making.
约 80%的成年人都会受到下背痛的影响,其中许多人会到全科医生处就诊。由于缺乏有效的治疗方法,为患者提供管理可能具有挑战性。国际临床实践指南广泛认为,应向患者提供有关其疼痛性质的信息,并建议他们尽管感到不适仍保持活跃。提供这些信息需要时间,而且在许多国家的全科医疗中,由于资源有限,这一过程受到挑战。此外,全科医疗的设置在规模和临床工作人员组成方面存在很大差异——这既带来了困难,也为开发替代临床管理方法提供了机会。通过让临床工作人员(除全科医生外)参与,增加患者就诊时间已被证明对其他疾病是可行的。我们建议将这种方法应用于非特异性下背痛。因此,我们建议让临床工作人员参与进来,作为全科医疗中管理下背痛的新策略的一部分。
如果基于理论并针对利益相关者进行调整,多方面实施策略有可能有效地改变全科医疗中对下背痛患者的临床管理。受医学研究委员会(Medical Research Council)对复杂干预措施的指导和 ChiPP(专业绩效变化)声明的启发,我们建议应用以下两个政策类别:组织变革(环境/社会规划)和服务提供。这将涉及关注环境结构调整、建模、赋能、教育、培训、劝说和激励全科医生,同时采取一项总体策略,即让临床工作人员参与下背痛的管理。
这是一个支持在全科医疗中为下背痛患者提供循证治疗的多方面策略的临床前建议。作为一个原创想法,我们建议让临床工作人员参与向患者提供信息和建议是可行的,而全科医生仍负责做出诊断决策。