Yano Takao, Kawana Ryo, Yamauchi Koichiro, Endo George, Nagamine Yasuhiro
Department of Emergency Center and Critical Care Medicine, Miyazaki Prefectural Nobeoka Hospital, Japan.
Department of Emergency Center, Miyazaki Prefectural Nobeoka Hospital, Japan.
Intern Med. 2019 Jun 15;58(12):1713-1721. doi: 10.2169/internalmedicine.1932-18. Epub 2019 Feb 25.
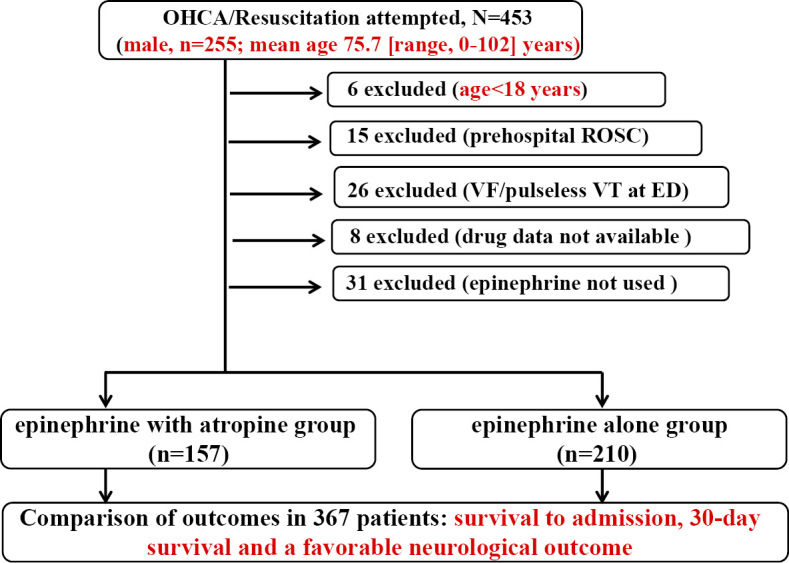
Objective The updated guidelines of 2015 for cardiopulmonary resuscitation (CPR) do not recommend the routine use of atropine for cardiopulmonary arrest. Methods The study population included out-of-hospital cardiac arrest (OHCA) patients with non-shockable rhythm who were encountered at a Japanese community hospital between October 1, 2012 and April 30, 2017. Results At the outcome, the epinephrine with atropine and epinephrine-only groups had a similar survival rate to that at hospital admission (28.7% vs. 26.7%: p=0.723). The odds ratio (OR) for the survival to hospital admission after the administration of atropine with epinephrine was 1.33 (95% CI 1.09-1.62; p<0.01), while that after the administration of epinephrine was 0.64 (95% CI: 0.55-0.74, p<0.01). The ORs for the survival to hospital admission for patients with pulseless electrical activity in the epinephrine-alone group and the atropine with epinephrine group were 0.62 (95% CI 0.49-0.78; p<0.01) and 1.35 (95% CI 0.99-1.83; p=0.06), respectively, and those for such patients with asystole in the epinephrine-alone group and the atropine with epinephrine group were 0.64 (95% CI 0.53-0.76; p<0.01) and 1.39 (95% CI 1.10-1.77; p<0.01), respectively. The OR for the survival to hospital admission after the administration of atropine sulfate (1 mg) was 2.91 (95% CI 1.49-5.67; p<0.01), while that for the survival to hospital admission after the administration of 0, 2 and ≥3 mg atropine sulfate was 0.38 (95% CI 0.29-0.50; p<0.01), 1.54 (95% CI 0.58-4.08; p=0.38) and 0.23 (95% CI 0.09-0.60; p<0.01), respectively. Conclusion The addition of atropine (within 2 mg) following epinephrine was a comprehensive independent predictor of the survival to hospital admission for non-shockable (especially asystole) OHCA adults.
目的 2015 年心肺复苏(CPR)更新指南不建议对心脏骤停常规使用阿托品。方法 研究人群包括 2012 年 10 月 1 日至 2017 年 4 月 30 日期间在日本一家社区医院遇到的非可电击心律的院外心脏骤停(OHCA)患者。结果 在结局方面,肾上腺素联合阿托品组和仅用肾上腺素组的入院生存率相似(28.7% 对 26.7%:p = 0.723)。肾上腺素联合阿托品给药后入院生存的比值比(OR)为 1.33(95%CI 1.09 - 1.62;p < 0.01),而仅用肾上腺素给药后的 OR 为 0.64(95%CI:0.55 - 0.74,p < 0.01)。仅用肾上腺素组和肾上腺素联合阿托品组中无脉电活动患者入院生存的 OR 分别为 0.62(95%CI 0.49 - 0.78;p < 0.01)和 1.35(95%CI 0.99 - 1.83;p = 0.06),仅用肾上腺素组和肾上腺素联合阿托品组中的心搏停止患者入院生存的 OR 分别为 0.64(95%CI 0.53 - 0.76;p < 0.01)和 1.39(95%CI 1.10 - 1.77;p < 0.01)。硫酸阿托品(1mg)给药后入院生存的 OR 为 2.91(95%CI 1.49 - 5.67;p < 0.01),而硫酸阿托品 0mg、2mg 和≥3mg 给药后入院生存的 OR 分别为 0.38(95%CI 0.29 - 0.50;p < 0.01)、1.54(95%CI 0.58 - 4.08;p = 0.38)和 0.23(95%CI 0.09 - 0.60;p < 0.01)。结论 肾上腺素后加用阿托品(2mg 以内)是不可电击心律(尤其是心搏停止)的 OHCA 成年患者入院生存的综合独立预测因素。