Department of Oncology, Chinese People's Liberation Army General Hospital, Beijing 100853, China.
Disinfection Supply Room, Chinese People's Liberation Army General Hospital, Beijing 100853, China.
Dis Markers. 2019 Jan 20;2019:6812045. doi: 10.1155/2019/6812045. eCollection 2019.
Previously, it was demonstrated that serum levels of tumor markers, CEA and CA19-9, correlated with chemotherapy. Consequently, it has been hypothesized that dynamic monitoring of changes in these markers may predict the shrinkage or growth of colorectal cancers. To test this hypothesis, we analyzed CEA and CA19-9 serum levels in patients with advanced colorectal cancer who received cetuximab in combination with chemotherapy. These levels were evaluated at various time points to identify their potential to serve as early efficacy predictors during treatment and early predictors of disease progression.
Measurements of tumor markers, CEA and CA 19-9, in patients with metastatic colorectal cancer ( = 73) who received cetuximab plus folinic acid, fluorouracil, and oxaliplatin or irinotecan (FOLFOX4/FOLFIRI) as a first-line treatment at our center were retrospectively analyzed. These levels were also compared with objective responses according to the World Health Organization criteria. Initially, 65 patients had elevated CEA levels (>5 ng/ml), and 59 patients had elevated levels of CA19-9 (>37 U/ml). A total of 172 cycles and 165 cycles of computed tomography/magnetic resonance imaging observations were available for review from these two patient groups.
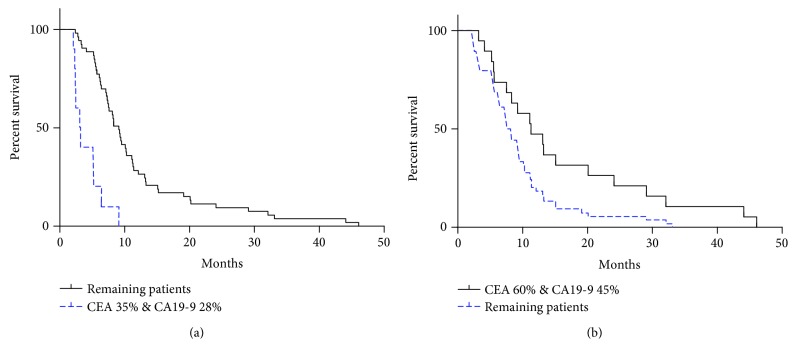
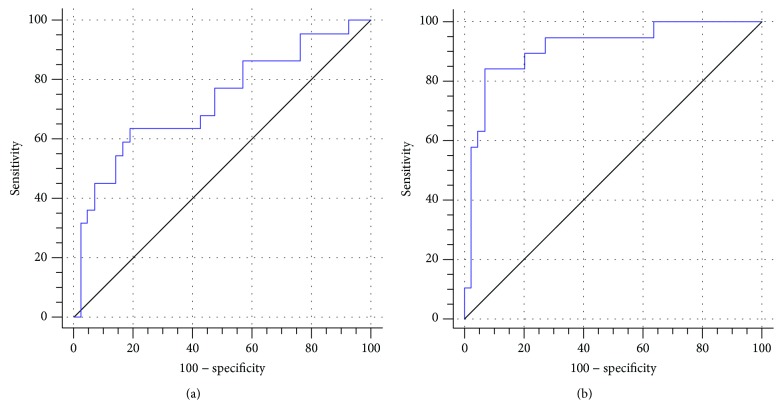
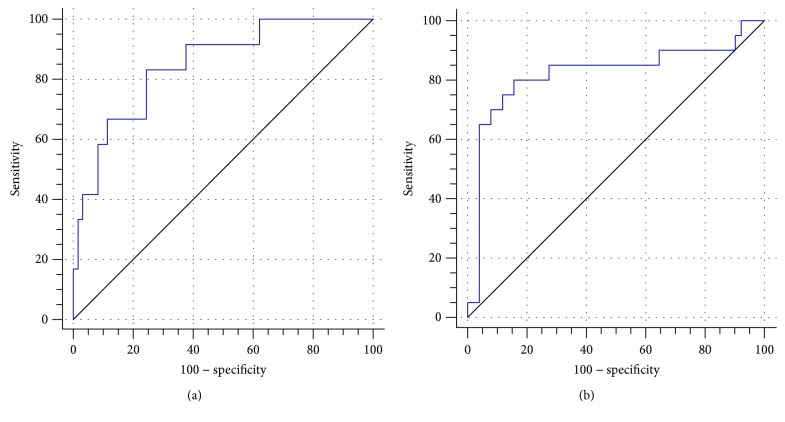
After completing three cycles of treatment, the best diagnosis of cetuximab resistance was achieved when CEA increased by 35% (efficacy, 83.33%; sensitivity, 75.41%) and when CA19-9 increased by 28% (efficacy, 80.00%; sensitivity, 84.31%). Next, the efficacy of cetuximab at the time of diagnosis (at the first imaging examination/after three cycles of treatment) was evaluated after the first cycle of chemotherapy. When CEA decreased by 60% from its baseline level, the best effective rate and sensitivity were observed (63.64% and 80.95%, respectively). Similarly, when CA19-9 was 45% lower than its baseline level, the best effective rate and sensitivity were observed (84.21% and 93.18%, respectively). To evaluate progression-free survival (PFS), levels of both CEA and CA19-9 were evaluated after the third cycle of chemotherapy. Increases of 35% and 28%, respectively, resulted in a shorter PFS period compared with the other patients (3.15 months vs. 9.10 months, respectively; < 0.0001). Conversely, when the evaluation was performed after the first cycle of chemotherapy, patients exhibiting a 60% decrease in CEA and a 45% decrease in CA19-9 had a longer PFS period (11.13 months vs. 8.10 months, respectively; = 0.0395).
CEA and CA19-9 are useful indicators of therapeutic curative effect from cetuximab combined with first-line chemotherapy. These markers also helped assess cetuximab resistance and served as early predictors of initial treatment effectiveness. Furthermore, a simultaneous increase or decrease in the levels of both indicators was consistent with the observed differences in PFS.
此前已经证实,肿瘤标志物 CEA 和 CA19-9 的血清水平与化疗相关。因此,人们假设动态监测这些标志物的变化可能可以预测结直肠癌的缩小或增长。为了验证这一假设,我们分析了接受西妥昔单抗联合化疗的晚期结直肠癌患者的 CEA 和 CA19-9 血清水平。在不同时间点评估这些水平,以确定其在治疗期间作为早期疗效预测指标和疾病进展早期预测指标的潜力。
回顾性分析了在我们中心接受西妥昔单抗联合亚叶酸钙、氟尿嘧啶和奥沙利铂或伊立替康(FOLFOX4/FOLFIRI)作为一线治疗的转移性结直肠癌(n=73)患者的肿瘤标志物 CEA 和 CA19-9 水平。这些水平也与根据世界卫生组织标准的客观反应进行了比较。最初,65 名患者的 CEA 水平升高(>5ng/ml),59 名患者的 CA19-9 水平升高(>37U/ml)。这两个患者组共有 172 个和 165 个周期的计算机断层扫描/磁共振成像观察可供审查。
完成三周期治疗后,当 CEA 增加 35%(疗效为 83.33%;灵敏度为 75.41%)和 CA19-9 增加 28%(疗效为 80.00%;灵敏度为 84.31%)时,对西妥昔单抗耐药性的最佳诊断得以实现。接下来,在第一次化疗后评估了西妥昔单抗在诊断时(第一次影像学检查/完成三个周期治疗后)的疗效。当 CEA 从基线水平下降 60%时,观察到最佳有效率和灵敏度(分别为 63.64%和 80.95%)。同样,当 CA19-9 比基线水平低 45%时,观察到最佳有效率和灵敏度(分别为 84.21%和 93.18%)。为了评估无进展生存期(PFS),在第三次化疗后评估了 CEA 和 CA19-9 的水平。分别增加 35%和 28%与其他患者相比,导致 PFS 期缩短(分别为 3.15 个月和 9.10 个月;<0.0001)。相反,当在第一次化疗后进行评估时,CEA 下降 60%和 CA19-9 下降 45%的患者 PFS 期更长(分别为 11.13 个月和 8.10 个月;=0.0395)。
CEA 和 CA19-9 是西妥昔单抗联合一线化疗治疗疗效的有用指标。这些标志物还有助于评估西妥昔单抗耐药性,并作为初始治疗效果的早期预测指标。此外,两个指标水平的同时升高或降低与观察到的 PFS 差异一致。