Han Kap Su, Kim Su Jin, Lee Eui Jung, Jung Jae Seung, Park Jae Hyoung, Lee Sung Woo
Department of Emergency Medicine, College of Medicine, Korea University, Seoul, Republic of Korea.
Department of Thoracic and Cardiovascular Surgery, College of Medicine, Korea University, Seoul, Republic of Korea.
Clin Cardiol. 2019 Apr;42(4):459-466. doi: 10.1002/clc.23169. Epub 2019 Mar 18.
Extracorporeal cardiopulmonary resuscitation (ECPR) is a method to improve survival outcomes in refractory cardiac arrest.
This study aimed to determine the associated factors related to outcome and to analyze the post-ECPR management in patients who received ECPR due to nonresponse to advanced cardiac life support (ACLS).
This was a retrospective analysis based on a prospective cohort. Cardiac arrest patients who received ECPR in our emergency department from May 2006 to December 2017 were selected from the prospective cohort. Patients who received ECPR for rearrest were excluded. The primary outcome was survival to discharge.
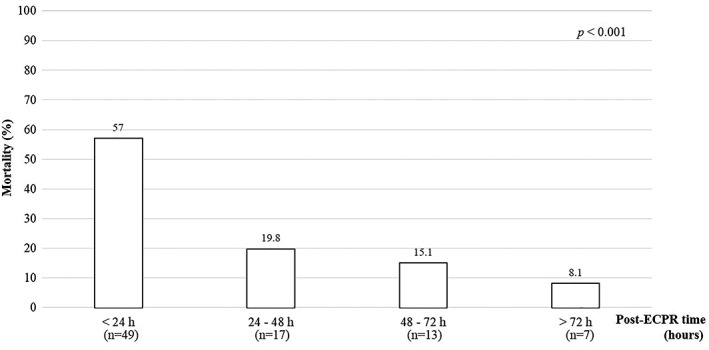
ECPR was attempted in 100 patients who did not respond to ACLS. Fourteen patients survived to discharge, and 12 (85.7%) patients showed good neurologic outcomes. The rate of survival to discharge decreased according to increasing age and ACLS duration. Age, presence of any return of spontaneous circulation (ROSC) during ACLS, and prolongation of ACLS were associated factors for survival discharge in ECPR patients. Fourteen patients required distal perfusion catheters, and 35 patients received continuous renal replacement therapy (CRRT). The proportion of death was the highest within 24 hours after ECPR as 57.0%.
The early transition from ACLS to ECPR may improve the ECPR outcomes. In addition, good outcomes are expected for ECPR performed after refractory arrest if the patient is young and experiences an ROSC event during ACLS. In post ECPR management, the majority of mortality events were occurred in the early period, and distal perfusion catheter and CRRT were frequently required.
体外心肺复苏(ECPR)是一种改善难治性心脏骤停患者生存结局的方法。
本研究旨在确定与结局相关的因素,并分析因对高级心脏生命支持(ACLS)无反应而接受ECPR的患者的ECPR后管理情况。
这是一项基于前瞻性队列的回顾性分析。从2006年5月至2017年12月在我院急诊科接受ECPR的心脏骤停患者中选取前瞻性队列。排除因再次心脏骤停接受ECPR的患者。主要结局是出院生存。
100例对ACLS无反应的患者尝试了ECPR。14例患者出院生存,其中12例(85.7%)神经功能结局良好。出院生存率随年龄增加和ACLS持续时间延长而降低。年龄、ACLS期间是否出现自主循环恢复(ROSC)以及ACLS延长是ECPR患者出院生存的相关因素。14例患者需要远端灌注导管,35例患者接受持续肾脏替代治疗(CRRT)。ECPR后24小时内死亡比例最高,为57.0%。
从ACLS早期过渡到ECPR可能改善ECPR结局。此外,如果患者年轻且在ACLS期间经历ROSC事件,难治性心脏骤停后进行ECPR有望获得良好结局。在ECPR后管理中,大多数死亡事件发生在早期,且经常需要远端灌注导管和CRRT。