Shimura Shunichi, Ogi Kazuhiro, Miyazaki Akihiro, Shimizu Shota, Kaneko Takeshi, Sonoda Tomoko, Kobayashi Junichi, Igarashi Tomohiro, Miyakawa Akira, Hasegawa Tadashi, Hiratsuka Hiroyoshi
Department of Oral Surgery, Sapporo Medical University School of Medicine, South 1 West 16, Chuo-ku, Sapporo 060-8543, Japan.
Department of Public Health, Sapporo Medical University School of Medicine, South 1 West 16, Chuo-ku, Sapporo 060-8543, Japan.
Cancers (Basel). 2019 Feb 25;11(2):269. doi: 10.3390/cancers11020269.
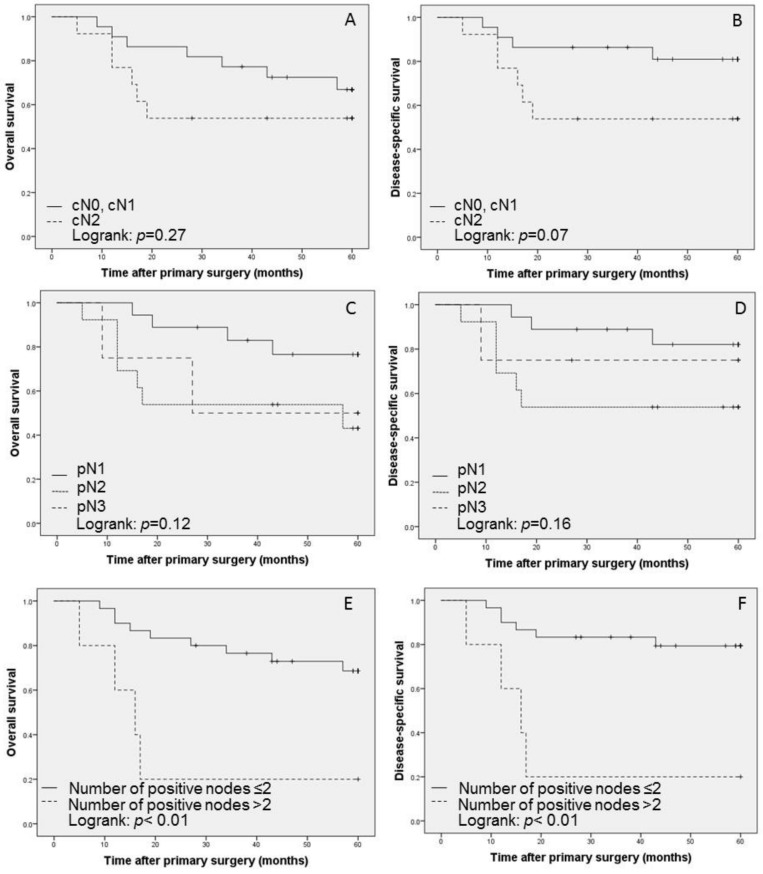
The most important prognostic factor in oral squamous cell carcinoma (OSCC) is neck metastasis, which is treated by neck dissection. Although selective neck dissection (SND) is a useful tool for clinically node-negative OSCC, its efficacy for neck node-positive OSCC has not been established. Sixty-eight OSCC patients with pN1⁻3 disease who were treated with curative surgery using SND and/or modified-radical/radical neck dissection (MRND/RND) were retrospectively reviewed. The neck control rate was 94% for pN1⁻3 patients who underwent SND. The five-year overall survival (OS) and disease-specific survival (DSS) in pN1-3 OSCC patients were 62% and 71%, respectively. The multivariate analysis of clinical and pathological variables identified the number of positive nodes as an independent predictor of SND outcome (OS, hazard ratio (HR) = 4.98, 95% confidence interval (CI): 1.48⁻16.72, < 0.01; DSS, HR = 6.44, 95% CI: 1.76⁻23.50, < 0.01). The results of this retrospective study showed that only SND for neck node-positive OSCC was appropriate for those with up to 2 lymph nodes that had a largest diameter ≤3 cm without extranodal extension (ENE) of the neck and adjuvant radiotherapy. However, the availability of postoperative therapeutic options for high-risk OSCC, including ENE and/or multiple positive lymph nodes, needs to be further investigated.
口腔鳞状细胞癌(OSCC)最重要的预后因素是颈部转移,通常通过颈部清扫术进行治疗。尽管选择性颈部清扫术(SND)对于临床淋巴结阴性的OSCC是一种有用的方法,但其对颈部淋巴结阳性的OSCC的疗效尚未确定。我们回顾性分析了68例接受SND和/或改良根治性/根治性颈部清扫术(MRND/RND)进行根治性手术治疗的pN1⁻3期OSCC患者。接受SND的pN1⁻3期患者的颈部控制率为94%。pN1-3期OSCC患者的五年总生存率(OS)和疾病特异性生存率(DSS)分别为62%和71%。对临床和病理变量的多因素分析确定阳性淋巴结数量是SND结果的独立预测因素(OS,风险比(HR)=4.98,95%置信区间(CI):1.48⁻16.72,<0.01;DSS,HR = 6.44,95%CI:1.76⁻23.50,<0.01)。这项回顾性研究的结果表明,对于颈部淋巴结阳性的OSCC患者,只有在最大直径≤3 cm的淋巴结不超过2个且无颈部结外侵犯(ENE)并接受辅助放疗的情况下,单纯SND才是合适的。然而,对于包括ENE和/或多个阳性淋巴结在内的高危OSCC,术后治疗选择的可用性仍需进一步研究。