British Medical Journal Technology Assessment Group (BMJ-TAG), BMA House, London, UK.
BMJ Open. 2019 Mar 1;9(3):e024691. doi: 10.1136/bmjopen-2018-024691.
To compare the effectiveness and safety of treatments for advanced or metastatic renal cell carcinoma (amRCC) after treatment with vascular endothelial growth factor (VEGF)-targeted treatment.
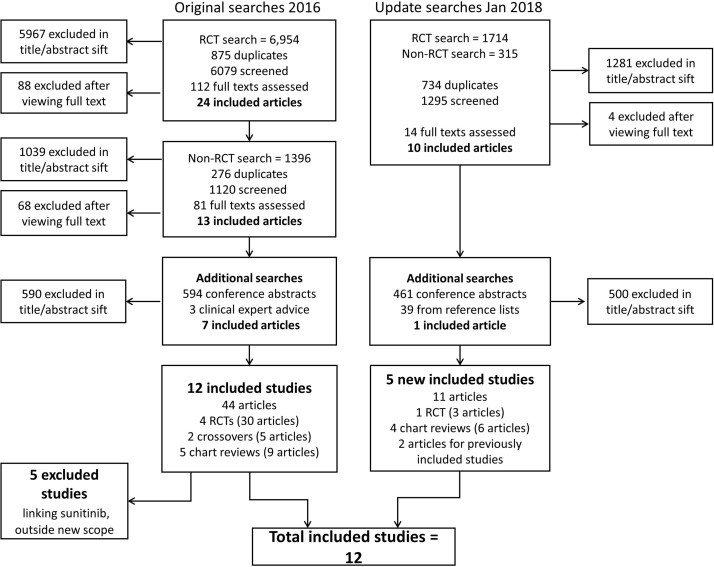
Systematic review and network meta-analysis of randomised controlled trials (RCTs) and comparative observational studies. MEDLINE, EMBASE and Cochrane Library were searched up to January 2018.
People with amRCC requiring treatment after VEGF-targeted treatment.
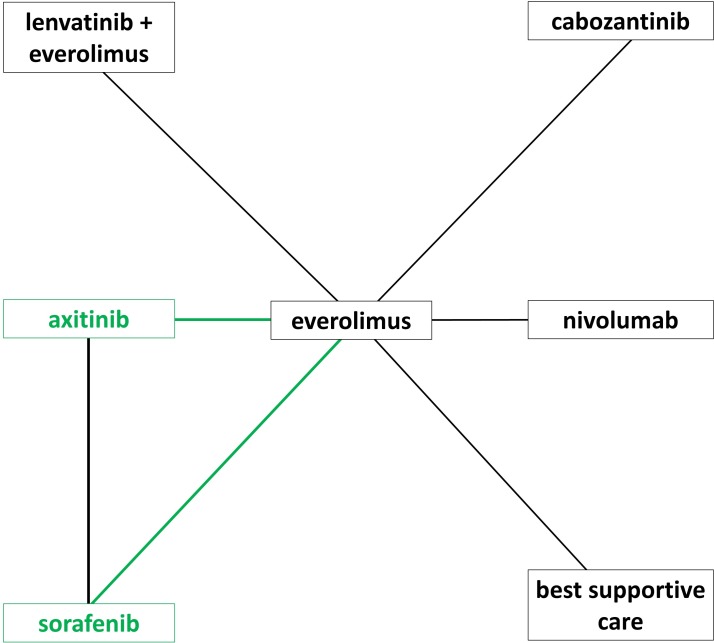
Axitinib, cabozantinib, everolimus, lenvatinib with everolimus, nivolumab, sorafenib and best supportive care (BSC).
Primary outcomes were overall survival (OS) and progression-free survival (PFS); secondary outcomes were objective response rate (ORR), adverse events, and health-related quality of life (HRQoL).
Twelve studies were included (n=5144): five RCTs and seven observational studies. Lenvatinib with everolimus significantly increased OS and PFS over everolimus (HR 0.61, 95% Credible Interval [95%CrI]: 0.36 to 0.96 and 0.47, 95%CrI: 0.26 to 0.77, respectively) as did cabozantinib (HR 0.66, 95%CrI: 0.53 to 0.82 and 0.51, 95%CrI: 0.41 to 0.63, respectively). This remained the case when observational evidence was included. Nivolumab also significantly improved OS versus everolimus (HR 0.74, 95%CrI: 0.57 to 0.93). OS sensitivity analysis, including observational studies, indicates everolimus being more effective than axitinib and sorafenib. However, inconsistency was identified in the OS sensitivity analysis. PFS sensitivity analysis suggests axitinib is more effective than everolimus, which may be more effective than sorafenib. The results for ORR supported the OS and PFS analyses. Nivolumab is associated with fewer grade 3 or grade 4 adverse events than lenvatinib with everolimus or cabozantinib. HRQoL could not be analysed due to differences in tools used.
Lenvatinib with everolimus, cabozantinib and nivolumab are effective in prolonging the survival for people with amRCC subsequent to VEGF-targeted treatment, but there is considerable uncertainty about how they compare to each other and how much better they are than axitinib and sorafenib.
CRD42017071540.
比较血管内皮生长因子(VEGF)靶向治疗后晚期或转移性肾细胞癌(amRCC)患者的治疗效果和安全性。
对随机对照试验(RCT)和比较观察性研究进行系统评价和网络荟萃分析。检索了 MEDLINE、EMBASE 和 Cochrane 图书馆,检索日期截至 2018 年 1 月。
需要在 VEGF 靶向治疗后进行治疗的 amRCC 患者。
阿昔替尼、卡博替尼、依维莫司、仑伐替尼联合依维莫司、纳武单抗、索拉非尼和最佳支持治疗(BSC)。
主要结局为总生存(OS)和无进展生存(PFS);次要结局为客观缓解率(ORR)、不良事件和健康相关生活质量(HRQoL)。
共纳入 12 项研究(n=5144):5 项 RCT 和 7 项观察性研究。与依维莫司相比,仑伐替尼联合依维莫司显著提高了 OS(HR 0.61,95%可信区间[95%CrI]:0.36 至 0.96)和 PFS(HR 0.47,95%CrI:0.26 至 0.77),卡博替尼也有相似的结果(HR 0.66,95%CrI:0.53 至 0.82 和 0.51,95%CrI:0.41 至 0.63)。纳入观察性证据后,这一结果仍然成立。与依维莫司相比,纳武单抗也显著提高了 OS(HR 0.74,95%CrI:0.57 至 0.93)。OS 敏感性分析包括观察性研究,表明依维莫司比阿昔替尼和索拉非尼更有效。然而,OS 敏感性分析中存在不一致性。PFS 敏感性分析表明阿昔替尼比依维莫司更有效,而依维莫司可能比索拉非尼更有效。ORR 的结果支持 OS 和 PFS 分析。与仑伐替尼联合依维莫司或卡博替尼相比,纳武单抗与较少的 3 级或 4 级不良事件相关。由于使用的工具不同,无法进行 HRQoL 分析。
在 VEGF 靶向治疗后,仑伐替尼联合依维莫司、卡博替尼和纳武单抗可延长晚期或转移性肾细胞癌患者的生存时间,但在这些治疗方法相互比较以及与阿昔替尼和索拉非尼相比时,存在相当大的不确定性。
PROSPERO 注册号:CRD42017071540。