School of Life Sciences, Arizona State University, PO Box 874501, Tempe, AZ, 85287-4501, USA.
Center for Personalized Diagnostics, The Biodesign Institute, Arizona State University, Tempe, AZ, USA.
BMC Cancer. 2019 Mar 4;19(1):200. doi: 10.1186/s12885-019-5402-1.
Cancer immunotherapy with immune checkpoint blockade (CKB) is now standard of care for multiple cancers. The clinical response to CKB is associated with T cell immunity targeting cancer-induced mutations that generate novel HLA-binding epitopes (neoepitopes).
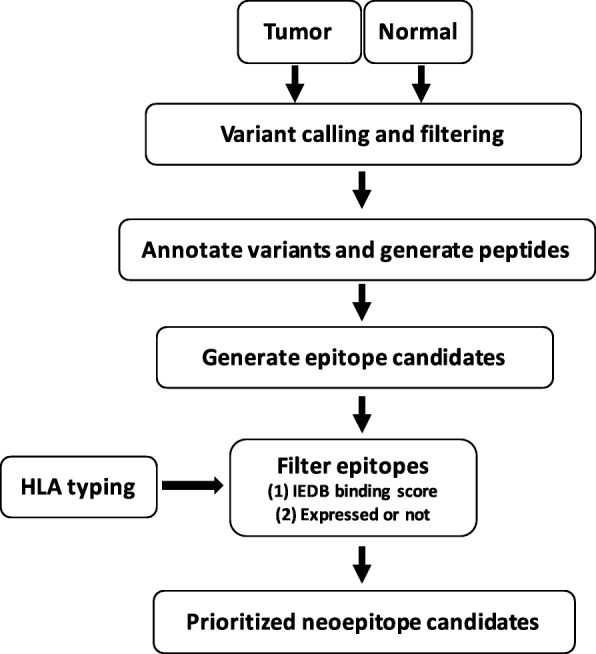
Here, we developed a rapid bioinformatics pipeline and filtering strategy, EpitopeHunter, to identify and prioritize clinically relevant neoepitopes from the landscape of somatic mutations. We used the pipeline to determine the frequency of neoepitopes from the TCGA dataset of invasive breast cancers. We predicted HLA class I-binding neoepitopes for 870 breast cancer samples and filtered the neoepitopes based on tumor transcript abundance.
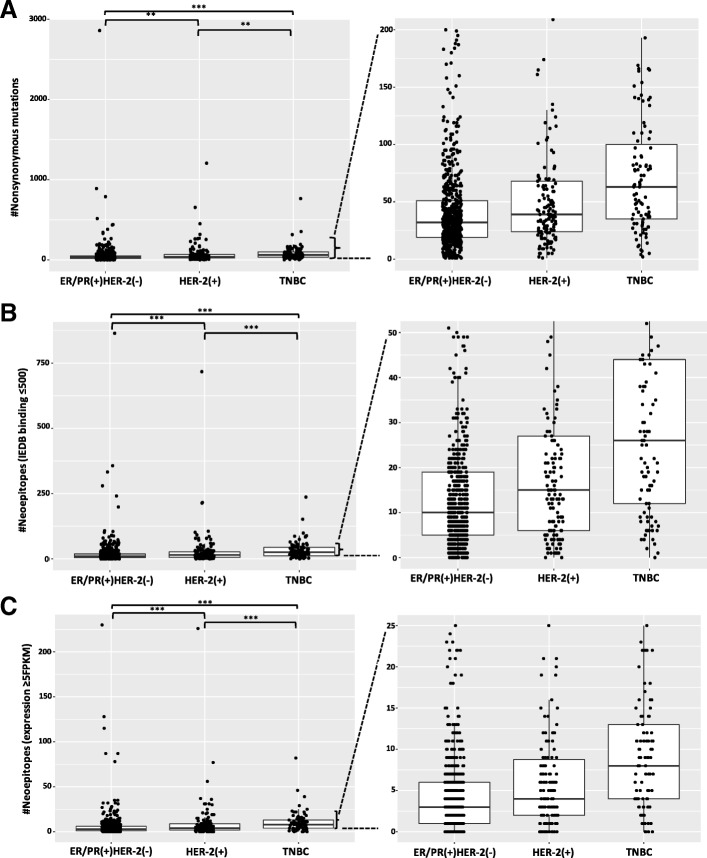
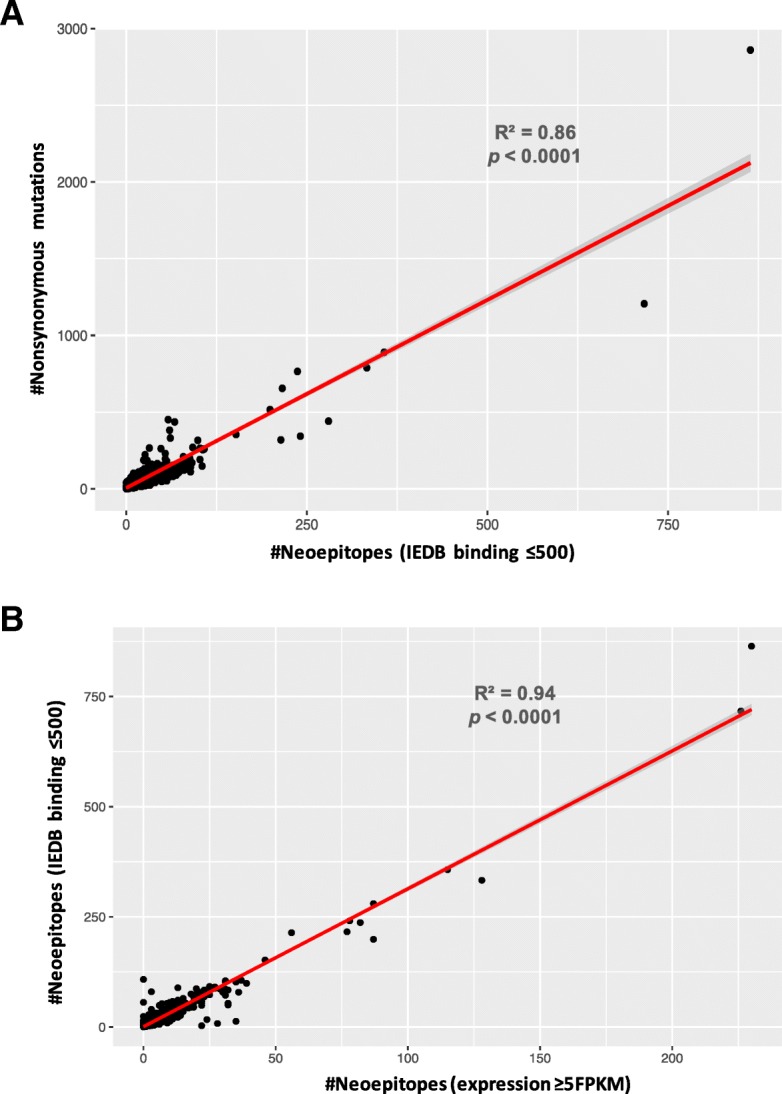
We found that the total mutational burden (TMB) was highest for triple-negative breast cancer, TNBC, (median = 63 mutations, range: 2-765); followed by HER-2(+) (median = 39 mutations, range: 1-1206); and lowest for ER/PR(+)HER-2(-) (median = 32 mutations, range: 1-2860). 40% of the nonsynonymous mutations led to the generation of predicted neoepitopes. The neoepitope load (NEL) is highly correlated with the mutational burden (R = 0.86).
Only half (51%) of the predicted neoepitopes are expressed at the RNA level (FPKM≥2), indicating the importance of assessing whether neoepitopes are transcribed. However, of all patients, 93% have at least one expressed predicted neoepitope, indicating that most breast cancer patients have the potential for neo-epitope targeted immunotherapy.
免疫检查点阻断(CKB)的癌症免疫疗法现已成为多种癌症的标准治疗方法。CKB 的临床反应与靶向癌症诱导突变的 T 细胞免疫有关,这些突变会产生新的 HLA 结合表位(新表位)。
在这里,我们开发了一种快速的生物信息学管道和过滤策略,EpitopeHunter,用于从体细胞突变景观中识别和优先考虑临床相关的新表位。我们使用该管道来确定来自 TCGA 浸润性乳腺癌数据集的新表位频率。我们预测了 870 个乳腺癌样本的 HLA Ⅰ类结合新表位,并根据肿瘤转录物丰度对新表位进行了过滤。
我们发现,三阴性乳腺癌(TNBC)的总突变负担(TMB)最高(中位数=63 个突变,范围:2-765);其次是 HER-2(+)(中位数=39 个突变,范围:1-1206);ER/PR(+)HER-2(-)最低(中位数=32 个突变,范围:1-2860)。40%的非同义突变导致了预测新表位的产生。新表位负荷(NEL)与突变负担高度相关(R=0.86)。
只有一半(51%)的预测新表位在 RNA 水平上表达(FPKM≥2),这表明评估新表位是否转录的重要性。然而,所有患者中有 93%至少有一个表达的预测新表位,这表明大多数乳腺癌患者具有针对新表位的免疫治疗潜力。