Harvard University, 677 Huntington Ave, Kresge Building, Room 506G, Boston, MA, 02115, USA.
Harvard T.H. Chan School of Public Health, 677 Huntington Ave, Kresge Building, Room 506G, Boston, MA, 02115, USA.
BMC Infect Dis. 2019 Mar 5;19(1):227. doi: 10.1186/s12879-019-3833-6.
There is great interest in the use of reduced dosing schedules for pneumococcal conjugate vaccines, a strategy premised on maintaining an acceptable level of protection against disease and carriage of the organism. We asked about the practicality of measuring differential effectiveness against carriage in a population with and without widespread use of the vaccine for infants.
We adapted an existing transmission-dynamic, individual-based stochastic model fitted to the prevaccine epidemiology of pneumococcal carriage in the United States, and compared the observed vaccine-type carriage prevalence in different arms of a simulated trial with one, two, or three infant doses plus a 12-month booster. Using these simulations, we calculated vaccine efficacy that would be estimated at different times post-enrollment in the trial and calculated required sample sizes to see a difference in carriage prevalence.
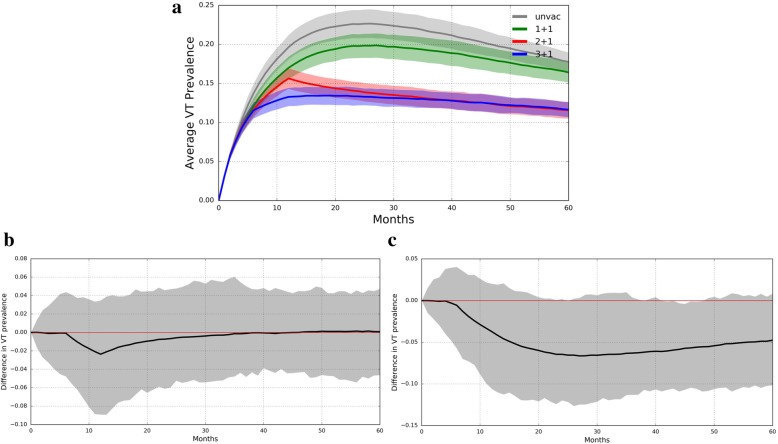
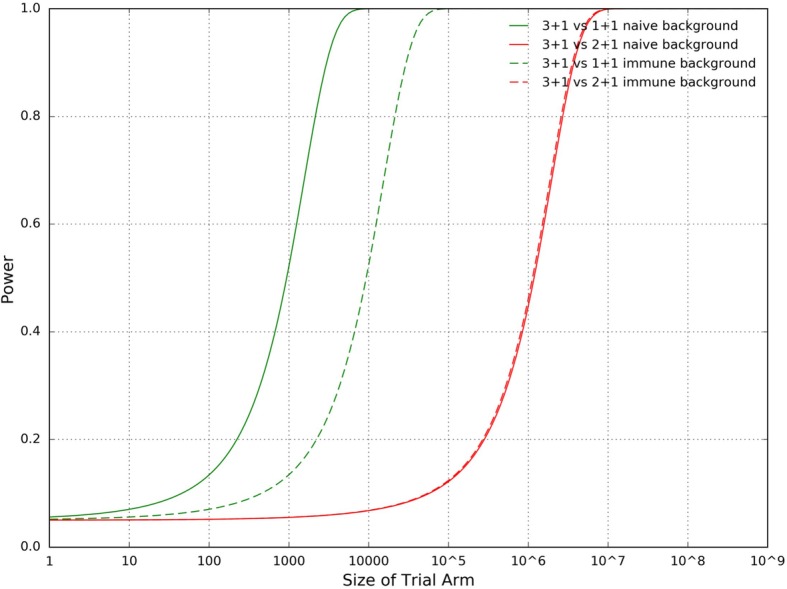
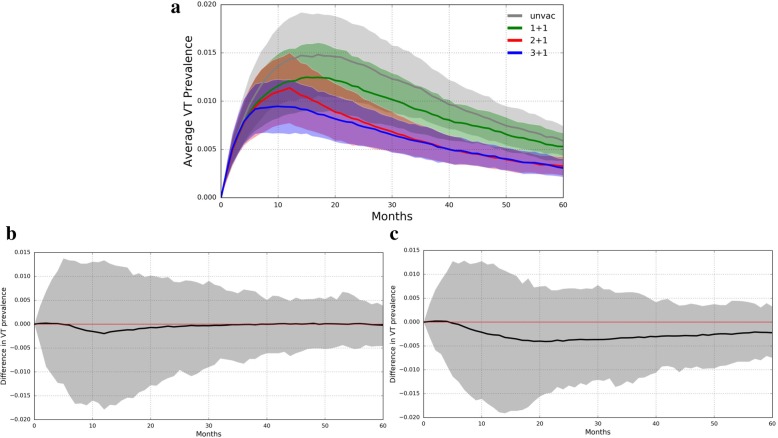
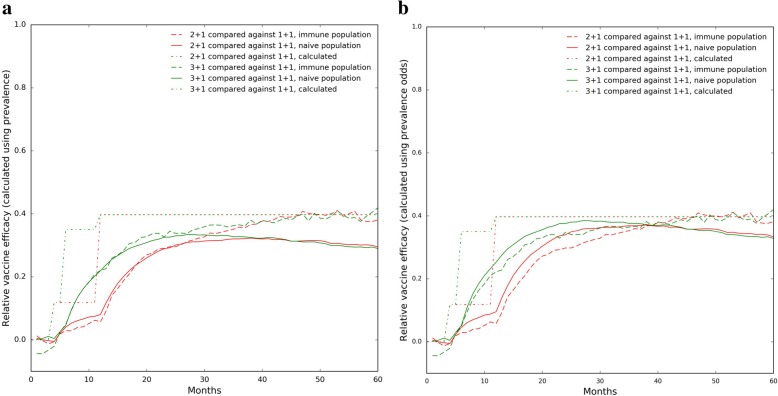
In a pneumococcal conjugate vaccine (PCV)-naïve population, the difference in vaccine-type (VT) pneumococcal carriage prevalence between trial arms was less than 7% and varied with sampling time. In a population already receiving routine PCV administration, VT pneumococcal prevalence is nearly indistinguishable between trial arms. Relative efficacy of different dosing schedules was strongly dependent on the time between enrollment and sampling, with maximal prevalence differences reached 1-3 years post-enrollment. Moreover, vaccine efficacy estimates were typically slightly higher in trials in communities already receiving vaccination. Despite this, much larger sample sizes-by more than an order of magnitude-are required for a vaccine trial conducted in a population receiving routine PCV administration as compared to in a PCV-naïve population.
These findings highlight some underappreciated aspects of clinical trials of pneumococcal conjugate vaccines with efficacy endpoints, such as the context- and time-dependence of efficacy estimates. They support the wisdom of conducting comparative dose schedule trials of conjugate vaccine effects on carriage in vaccine-naïve populations.
人们对使用减少剂量的肺炎球菌结合疫苗方案很感兴趣,这种策略的前提是保持对疾病和该病原体携带的可接受的保护水平。我们询问了在广泛为婴儿使用疫苗的人群中,测量针对携带的差异效力的实际情况。
我们改编了现有的基于传输动力学的个体随机模型,该模型适用于美国肺炎球菌携带的疫苗前流行病学,并比较了模拟试验中不同组别的观察到的疫苗型携带率,这些组别包括使用一、二或三剂婴儿疫苗加 12 个月加强针。使用这些模拟,我们计算了在试验登记后的不同时间估计的疫苗效力,并计算了观察携带率差异所需的样本量。
在肺炎球菌结合疫苗(PCV)初免人群中,试验组之间的疫苗型(VT)肺炎球菌携带率差异小于 7%,并且随采样时间而变化。在已经常规接种 PCV 的人群中,试验组之间的 VT 肺炎球菌流行率几乎无法区分。不同剂量方案的相对效力强烈依赖于登记和采样之间的时间,最大流行率差异在登记后 1-3 年达到。此外,在已经接受疫苗接种的社区进行的试验中,疫苗效力估计通常略高。尽管如此,与在 PCV 初免人群中进行的疫苗试验相比,在已经常规接种 PCV 的人群中进行疫苗试验所需的样本量要大得多,相差超过一个数量级。
这些发现强调了使用肺炎球菌结合疫苗进行疗效终点临床试验的一些被低估的方面,例如效力估计的背景和时间依赖性。它们支持在疫苗初免人群中进行针对疫苗对携带效果的比较剂量方案试验的智慧。