Clinical Trial Centre, University of Leipzig, Leipzig, Germany.
Department of Cardiovascular Surgery, Universitats-Herzzentrum Freiburg Bad Krozingen GmbH, Bad Krozingen, Germany.
BMJ Open. 2019 Mar 4;9(3):e025488. doi: 10.1136/bmjopen-2018-025488.
Spinal cord injury (SCI) including permanent paraplegia constitutes a common complication after repair of thoracoabdominal aortic aneurysms. The staged-repair concept promises to provide protection by inducing arteriogenesis so that the collateral network can provide a robust blood supply to the spinal cord after intervention. Minimally invasive staged segmental artery coil embolisation (MISACE) has been proved recently to be a feasible enhanced approach to staged repair.
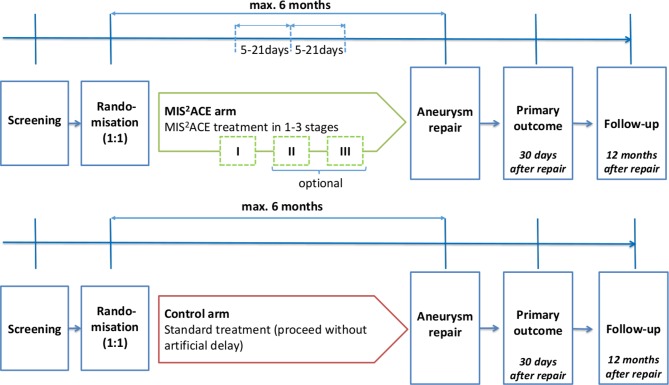
This randomised controlled trial uses a multicentre, multinational, parallel group design, where 500 patients will be randomised in a 1:1 ratio to standard aneurysm repair or to MISACE in 1-3 sessions followed by repair. Before randomisation, physicians document whether open or endovascular repair is planned. The primary endpoint is successful aneurysm repair without substantial SCI 30 days after aneurysm repair. Secondary endpoints include any form of SCI, mortality (up to 1 year), length of stay in the intensive care unit, costs and quality-adjusted life years. A generalised linear mixed model will be used with the logit link function and randomisation arm, mode of repair (open or endovascular repair), the Crawford type and the European System for Cardiac Operative Risk Evaluation (euroSCORE) II as fixed effects and the centre as a random effect. Safety endpoints include kidney failure, respiratory failure and embolic events (also from debris). A qualitative study will explore patient perceptions.
This trial has been approved by the lead Ethics Committee from the University of Leipzig (435/17-ek) and will be reviewed by each of the Ethics Committees at the trial sites. A dedicated project is coordinating communication and dissemination of the trial.
NCT03434314.
脊髓损伤(SCI)包括永久性截瘫,是胸主动脉腹主动脉瘤修复后的常见并发症。分期修复概念通过诱导动脉生成提供保护,以便在介入后侧支网络可以为脊髓提供充足的血液供应。最近已经证明微创分期节段性动脉线圈栓塞(MISACE)是一种可行的强化分期修复方法。
这项随机对照试验采用多中心、多国、平行分组设计,将 500 例患者随机分为 1:1 比例的标准动脉瘤修复组或 1-3 次 MISACE 组,然后进行修复。在随机分组之前,医生记录计划进行开放或血管内修复。主要终点是动脉瘤修复后 30 天无明显 SCI 的成功动脉瘤修复。次要终点包括任何形式的 SCI、死亡率(最长 1 年)、重症监护病房住院时间、成本和质量调整生命年。将使用广义线性混合模型,对数链接函数和随机分组臂、修复方式(开放或血管内修复)、Crawford 类型和欧洲心脏手术风险评估系统(euroSCORE)II 作为固定效应,中心作为随机效应。安全性终点包括肾衰竭、呼吸衰竭和栓塞事件(也来自碎片)。一项定性研究将探讨患者的认知。
该试验已获得莱比锡大学主要伦理委员会的批准(435/17-ek),并将由试验现场的每个伦理委员会进行审查。一个专门的项目正在协调试验的沟通和传播。
NCT03434314。