Department of Nephrology, Zhejiang Provincial People's Hospital, Zhejiang, 310014, P. R. China.
People's Hospital of Hangzhou Medical College, Zhejiang, 310014, P. R. China.
Sci Rep. 2019 Mar 5;9(1):3540. doi: 10.1038/s41598-019-39735-9.
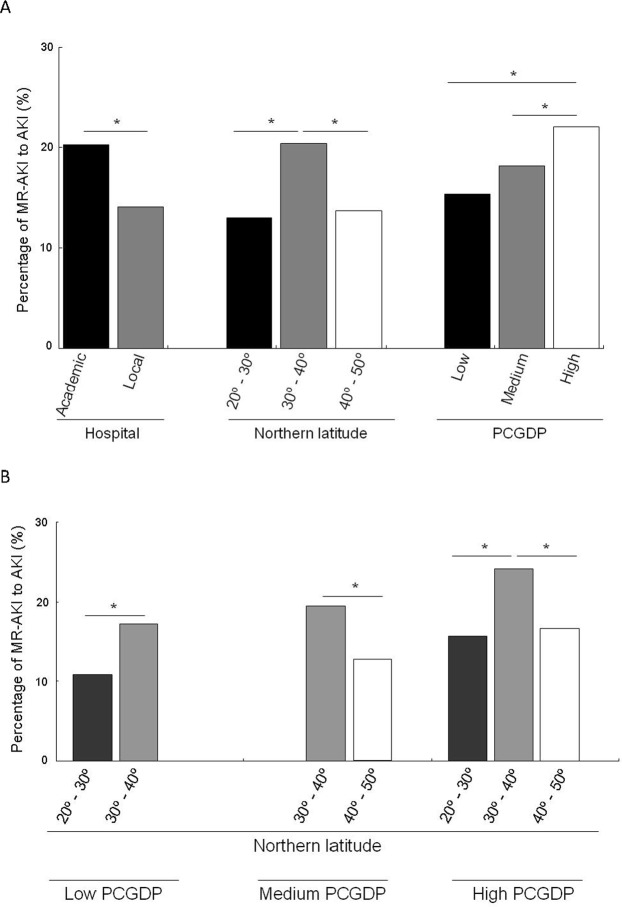
Cancer patients have a high risk for acute kidney injury (AKI); however, the incidence, severity, and risk factors of malignancy-related AKI (MR-AKI) are unclear. This study aimed to assess MR-AKI risk factors and provide reliable data for AKI prevention, diagnosis, and management in China. This cross-sectional study analysed data from 44 academic and local hospitals in China. AKI patients were identified based on 2 screening criteria: the 2012 Kidney Disease: Improving Global Outcomes-AKI definition and the expanded screening criteria for patients with no repeated serum creatinine (SCr) test within 7 days and those who recovered from AKI. Patients whose SCr level increased or decreased by 50% during hospitalization, compared with that at admission, were considered to have AKI according to the expanded criteria. A total of 7,604 AKI patients were enrolled (1,418 with MR-AKI). Patient characteristics were compared between the MR-AKI and non-MR-AKI groups. Multivariate logistic models were used to statistically assess risk factors. The proportions of MR-AKI patients in academic and local hospitals were 20.2% and 14.1%, respectively. The incidence of MR-AKI was higher in mid-China (the affluent region), elderly patients, and groups with higher per capita gross domestic product. Among MR-AKI cases, gastrointestinal cancer (50.1%) was the most common malignancy, followed by cancers of the reproductive (15.3%), haematological (13.1%), respiratory (11.8%), and other systems (8.3%), and cancers of unknown classification (1.4%). Of 268 hospital deaths, respiratory, haematological, gastrointestinal, reproductive, other system, and unknown classification cancers accounted for 29.3%, 18.8%, 18.6%, 12.9%, 16.9%, and 20.0%, respectively. Increased age, advanced AKI stage at peak, level of per capita gross domestic product, geographic region, and renal replacement therapy indication were risk factors for hospital mortality in patients with gastrointestinal MR-AKI, whereas cardiovascular disease history, AKI stage at peak, and geographic region were risk factors for mortality in patients with reproductive MR-AKI. The incidence and mortality of MR-AKI vary by hospital, economic level, age, geographic region, and malignancy type. High MR-AKI incidence was associated with gastrointestinal cancers and higher level of medical care provided by academic hospitals in affluent regions such as Beijing, Shanghai, and other provincial-level cities. Elderly patients with advanced gastrointestinal cancer in mid-China showed the highest incidence of MR-AKI and in-hospital mortality, and thus require special attention.
癌症患者发生急性肾损伤(AKI)的风险较高;然而,恶性肿瘤相关 AKI(MR-AKI)的发生率、严重程度和危险因素尚不清楚。本研究旨在评估 MR-AKI 的危险因素,为中国 AKI 的预防、诊断和管理提供可靠数据。本横断面研究分析了来自中国 44 家学术和地方医院的数据。AKI 患者的识别基于 2 个筛选标准:2012 年肾脏病:改善全球结局 AKI 定义和无重复血清肌酐(SCr)检测且 AKI 恢复患者的扩展筛选标准,在 7 天内。根据扩展标准,住院期间 SCr 水平增加或减少 50%的患者被认为患有 AKI。根据扩展标准,与入院时相比,住院期间 SCr 水平增加或减少 50%的患者被认为患有 AKI。共纳入 7604 例 AKI 患者(1418 例为 MR-AKI)。比较 MR-AKI 组和非 MR-AKI 组患者的特征。多变量逻辑模型用于统计评估危险因素。学术医院和地方医院的 MR-AKI 患者比例分别为 20.2%和 14.1%。在中国中部(富裕地区)、老年患者和人均国内生产总值较高的人群中,MR-AKI 的发生率较高。在 MR-AKI 病例中,胃肠道癌(50.1%)是最常见的恶性肿瘤,其次是生殖系统(15.3%)、血液系统(13.1%)、呼吸系统(11.8%)和其他系统(8.3%),以及未知分类(1.4%)癌症。在 268 例住院死亡中,呼吸系统、血液系统、胃肠道、生殖系统、其他系统和未知分类癌症分别占 29.3%、18.8%、18.6%、12.9%、16.9%和 20.0%。年龄较大、峰值时 AKI 分期较高、人均国内生产总值、地理区域和肾脏替代治疗指征是胃肠道 MR-AKI 患者住院死亡的危险因素,而心血管疾病史、峰值时 AKI 分期和地理区域是生殖系统 MR-AKI 患者死亡的危险因素。MR-AKI 的发生率和死亡率因医院、经济水平、年龄、地理区域和恶性肿瘤类型而异。高 MR-AKI 发生率与胃肠道癌症有关,并且北京、上海等省级城市等富裕地区的学术医院提供的医疗水平较高。中国中部年龄较大的晚期胃肠道癌老年患者 MR-AKI 发生率和住院死亡率最高,因此需要特别关注。