1 Graduate School of Medical Science and Engineering Korea Advanced Institute of Science and Technology Daejeon Republic of Korea.
2 Cardiovascular Center Division of Cardiology Seoul National University Bundang Hospital Seongnam Republic of Korea.
J Am Heart Assoc. 2019 Mar 19;8(6):e011077. doi: 10.1161/JAHA.118.011077.
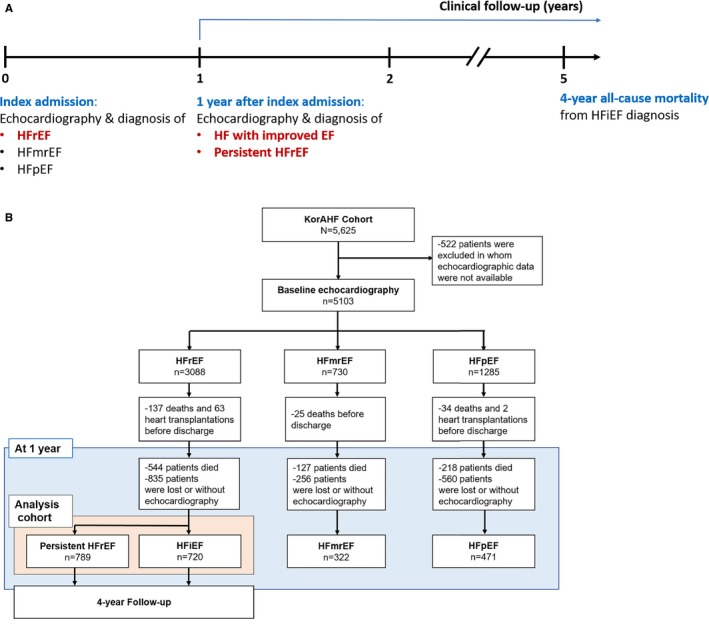
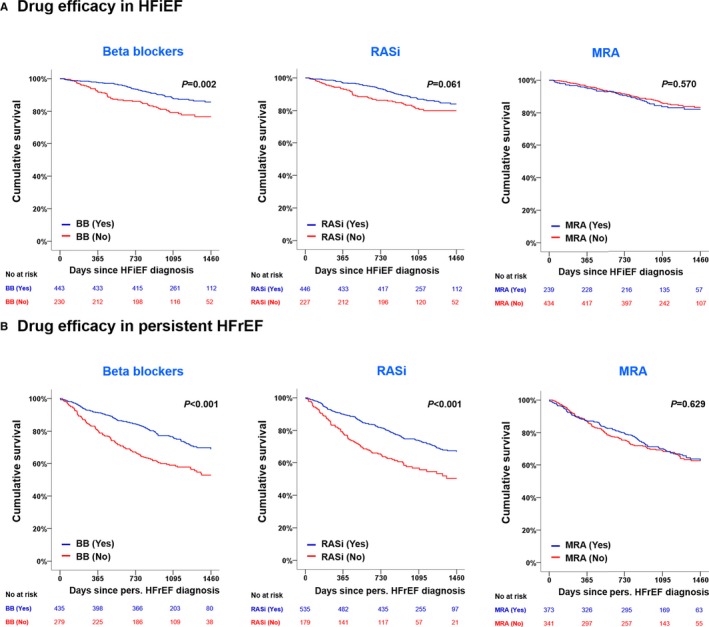
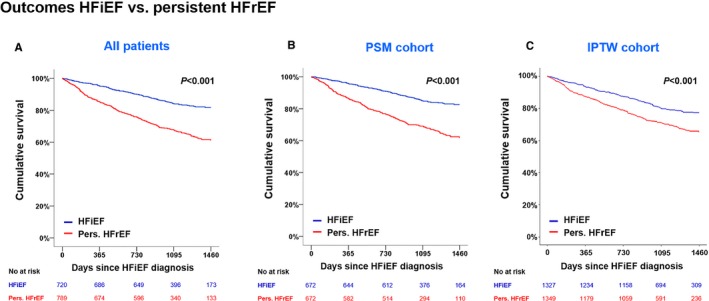
Background Many patients with heart failure ( HF ) with reduced ejection fraction ( HF r EF ) experience improvement or recovery of left ventricular ejection fraction ( LVEF ). Data on clinical characteristics, outcomes, and medical therapy in patients with HF with improved ejection fraction (HFiEF) are scarce. Methods and Results Of 5625 consecutive patients hospitalized for acute HF in the KorAHF (Registry [Prospective Cohort] for Heart Failure in Korea) study, 5103 patients had baseline echocardiography and 2302 patients had follow-up echocardiography at 12 months. HF phenotypes were defined as persistent HF r EF ( LVEF ≤40% at baseline and at 1-year follow-up), HF i EF ( LVEF ≤40% at baseline and improved up to 40% at 1-year follow-up), HF with midrange ejection fraction (LVEF between 40% and <50%), and HF with preserved ejection fraction ( LVEF ≥50%). The primary outcome was 4-year all-cause mortality from the time of HF i EF diagnosis. Among 1509 HF r EF patients who had echocardiography 1 year after index hospitalization, 720 (31.3%) were diagnosed as having HF i EF . Younger age, female sex, de novo HF , hypertension, atrial fibrillation, and β-blocker use were positive predictors and diabetes mellitus and ischemic heart disease were negative predictors of HF i EF . During 4-year follow-up, patients with HF i EF showed lower mortality than those with persistent HF r EF in univariate, multivariate, and propensity-score-matched analyses. β-Blockers, but not renin-angiotensin system inhibitors or mineralocorticoid receptor antagonists, were associated with a reduced all-cause mortality risk (hazard ratio: 0.59; 95% CI , 0.40-0.87; P=0.007). Benefits for outcome seemed similar among patients receiving low- or high-dose β-blockers (log-rank, P=0.304). Conclusions HF i EF is a distinct HF phenotype with better clinical outcomes than other phenotypes. The use of β-blockers may be beneficial for these patients. Clinical Trial Registration URL : https://www.clinicaltrials.gov . Unique identifier: NCT01389843.
许多射血分数降低的心力衰竭(HF rEF)患者的左心室射血分数(LVEF)会有所改善或恢复。目前有关射血分数改善的心力衰竭(HFiEF)患者的临床特征、结局和药物治疗的数据十分有限。
在 KorAHF(韩国心力衰竭注册研究[前瞻性队列研究])研究中,连续纳入 5625 例因急性心力衰竭住院的患者,其中 5103 例患者在基线和 12 个月时进行了基线超声心动图检查,2302 例患者进行了 12 个月的随访超声心动图检查。心力衰竭表型定义为持续性射血分数降低的心力衰竭(HF rEF,基线和 1 年随访时 LVEF ≤40%)、射血分数改善的心力衰竭(HF i EF,基线时 LVEF ≤40%,但在 1 年随访时增加至 40%)、射血分数中间范围的心力衰竭(LVEF 在 40%和<50%之间)和射血分数保留的心力衰竭(HFpEF,LVEF ≥50%)。主要结局是从 HF i EF 诊断开始的 4 年全因死亡率。在 1509 例接受指数住院后 1 年超声心动图检查的 HF rEF 患者中,有 720 例(31.3%)被诊断为 HF i EF。年龄较小、女性、新发心力衰竭、高血压、心房颤动和β受体阻滞剂的使用是 HF i EF 的阳性预测因素,而糖尿病和缺血性心脏病是 HF i EF 的阴性预测因素。在 4 年的随访中,与持续性 HF rEF 相比,HF i EF 患者的死亡率在单变量、多变量和倾向评分匹配分析中均较低。β受体阻滞剂,但不是肾素-血管紧张素系统抑制剂或盐皮质激素受体拮抗剂,与降低全因死亡风险相关(风险比:0.59;95%CI,0.40-0.87;P=0.007)。接受低剂量或高剂量β受体阻滞剂的患者的获益似乎相似(对数秩检验,P=0.304)。
HF i EF 是一种独特的心力衰竭表型,其临床结局优于其他表型。β受体阻滞剂的使用可能对这些患者有益。