Oregon Health & Science University, Portland.
University of California, San Francisco.
Arthritis Rheumatol. 2019 Jul;71(7):1101-1111. doi: 10.1002/art.40866. Epub 2019 May 28.
The natural history of nonradiographic axial spondyloarthritis (SpA) is incompletely characterized, and there are concerns that nonsteroidal antiinflammatory drugs provide inadequate disease control in patients with active disease. This study was undertaken to investigate the effects of certolizumab pegol (CZP), an anti-tumor necrosis factor treatment, in patients with nonradiographic axial SpA with objective signs of inflammation.
In this ongoing parallel-group double-blind study, adults with active disease were recruited from 80 centers in Australia, Europe, North America, and Taiwan, and were randomized 1:1 to receive placebo or CZP (400 mg at weeks 0, 2, and 4, followed by 200 mg every 2 weeks) in addition to nonbiologic background medication (NBBM). Switching to open-label CZP (or other biologic) or making background medication changes was permitted at any point during the trial, although changes before week 12 were discouraged. The primary end point was the proportion of patients achieving major improvement (MI) (i.e., a ≥2.0-point decrease in the score from baseline or achievement of the lowest possible score [0.6]) in the Ankylosing Spondylitis Disease Activity Score (ASDAS) at week 52.
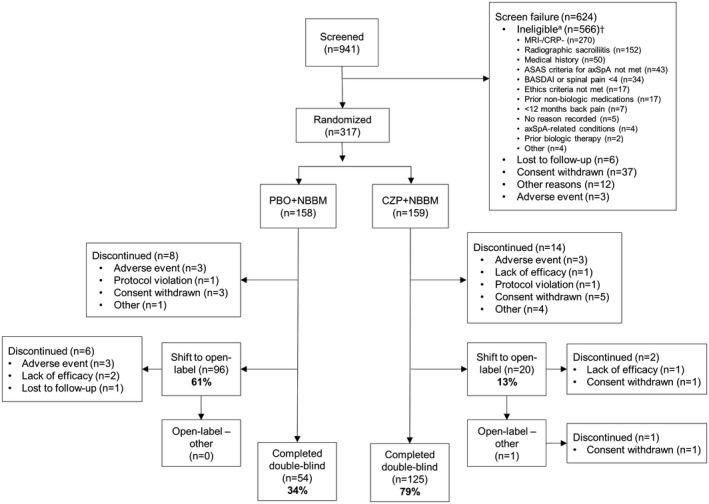
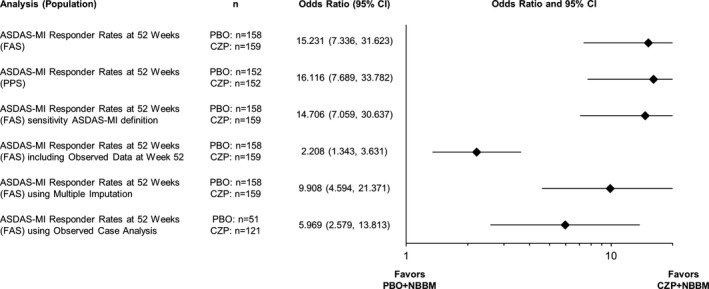
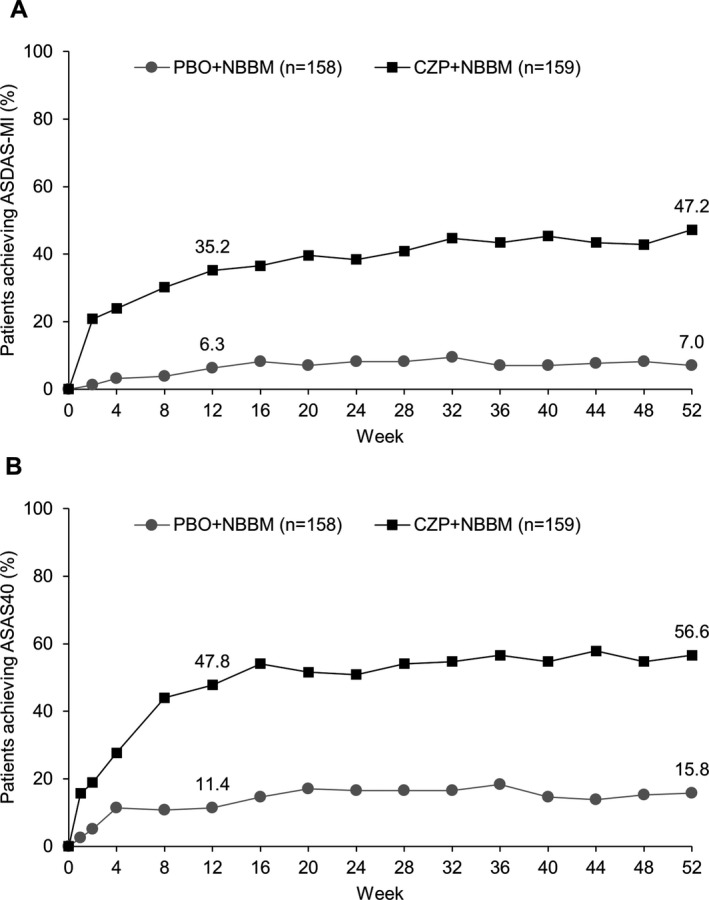
A total of 317 patients were randomized to receive placebo plus NBBM (n = 158) or CZP plus NBBM (n = 159). ASDAS-MI at week 52 was achieved in 47.2% (75 of 159) of CZP plus NBBM patients, which was significantly greater (P < 0.0001) than the 7.0% (11 of 158) of placebo plus NBBM patients in whom ASDAS-MI was achieved. Of the placebo plus NBBM patients, 60.8% (96 of 158) switched to open-label treatment before week 52 compared to 12.6% (20 of 159) of the CZP plus NBBM patients.
Adding CZP to background medication is superior to adding placebo in patients with active nonradiographic axial SpA. These results indicate that remission in nonradiographic axial SpA treated without biologics occurs infrequently, demonstrating the need for treatment beyond nonbiologic therapy.
非放射性轴性脊柱关节炎(SpA)的自然病史尚未完全阐明,人们担心在疾病活动期患者中,非甾体抗炎药不能充分控制疾病。本研究旨在探讨抗肿瘤坏死因子治疗药物培塞利珠单抗(CZP)在存在炎症客观指标的非放射性轴性 SpA 患者中的疗效。
在这项正在进行的平行分组双盲研究中,从澳大利亚、欧洲、北美和中国台湾的 80 个中心招募了疾病活动期的成年患者,并将其 1:1 随机分配至安慰剂组或 CZP 组(分别于第 0、2 和 4 周给予 400mg,然后每 2 周给予 200mg),同时接受非生物性背景治疗药物(NBBM)。在试验期间的任何时候都可以转换为开放标签 CZP(或其他生物制剂)或改变背景治疗药物,但在第 12 周之前不鼓励进行任何改变。主要终点是在第 52 周时,ASDAS 评分(Ankylosing Spondylitis Disease Activity Score)较基线下降≥2.0 分或达到最低可能评分(0.6)的患者比例(即取得主要改善(MI)的患者比例)。
共 317 例患者随机分为安慰剂+NBBM 组(n=158)或 CZP+NBBM 组(n=159)。在 CZP+NBBM 组中,有 47.2%(75/159)的患者在第 52 周时达到 ASDAS-MI,显著高于安慰剂+NBBM 组的 7.0%(11/158)。在安慰剂+NBBM 组中,有 60.8%(96/158)的患者在第 52 周前转换为开放标签治疗,而 CZP+NBBM 组中仅 12.6%(20/159)的患者转换为开放标签治疗。
在疾病活动期的非放射性轴性 SpA 患者中,添加 CZP 至背景治疗药物优于添加安慰剂。这些结果表明,未经生物制剂治疗的非放射性轴性 SpA 患者很少达到缓解,这表明需要在非生物治疗之外进行治疗。