IAME, UMR1137, INSERM, Paris Diderot University, Sorbonne Paris Cité, Paris, France.
Infectious and Tropical Diseases Department, Normandie Univ, UNICAEN, Normandie University Hospital, Caen, France.
PLoS One. 2019 Mar 13;14(3):e0213526. doi: 10.1371/journal.pone.0213526. eCollection 2019.
With HIV treatment as a prevention strategy, retention in care remains a key for sustained viral suppression. We sought to identify HIV-infected patients at risk for medical care interruption (MCI) in a high-income country.
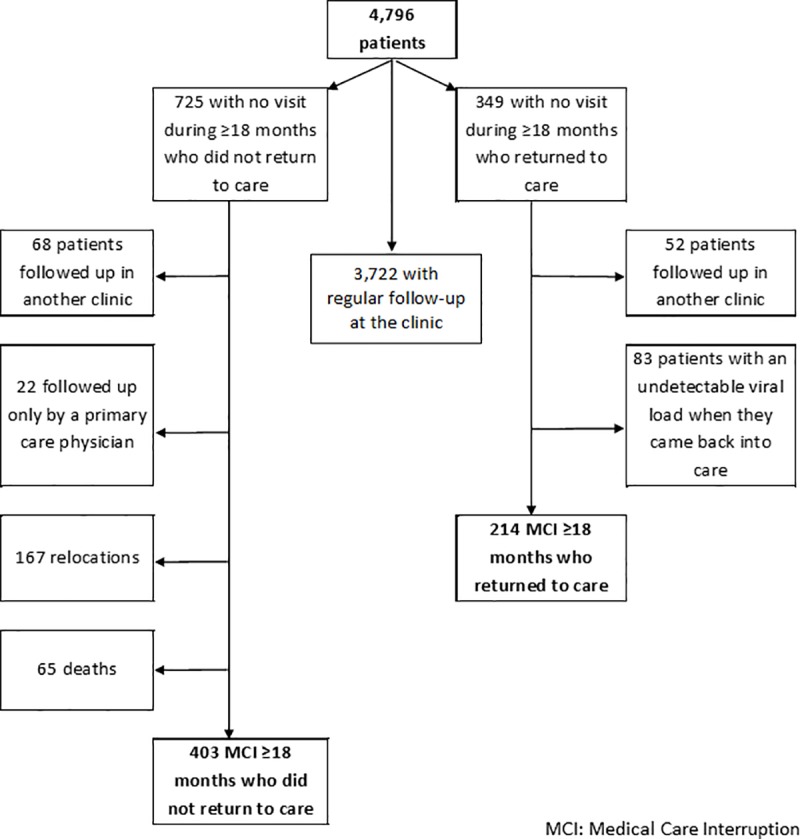
The HIV-infected patients enrolled had to attend the clinic at least twice between January 2010 and October 2014 and were followed up until May 2016. MCI was defined as patients not seeking care in or outside the clinic for at least 18 months, regardless of whether they returned to care after the interruption. The association between MCI and sociodemographic, clinical, and immuno-virological characteristics at HIV diagnosis and during follow-up was assessed using Cox models.
The incidence rate of MCI was 2.5 per 100 persons-years (95% confidence interval [CI] = 2.3-2.7). MCI was more likely in patients who accessed care >6 months after diagnosis (hazard ratio [HR] = 1.30, 95% CI = 1.10-1.54 vs. ≤6 months) or did not report a primary care physician (HR = 2.40; 95% CI = 2.03-2.84). MCI was less likely in patients born in sub-Saharan Africa (HR = 0.75, 95% CI = 0.62-0.91 vs. born in France). During follow-up, the risk of MCI increased when the last CD4 count was ≤350 (HR = 2.85, 95% CI = 2.02-4.04 vs. >500 cells/mm3) and when the patient was not on antiretroviral therapy (HR = 3.67, 95% CI = 2.90-4.66).
The incidence of MCI is low in this hospital that serves a large proportion of migrants. Low or no recorded CD4 counts for a medical visit could alert of a higher risk of MCI, even more in patients who accessed HIV care late or did not report a primary care physician.
随着 HIV 治疗成为预防策略,患者在治疗中的保留率仍然是持续病毒抑制的关键。我们旨在确定高收入国家中存在中断医疗护理风险(MCI)的 HIV 感染患者。
入组的 HIV 感染患者必须在 2010 年 1 月至 2014 年 10 月期间至少两次就诊于诊所,并在 2016 年 5 月之前进行随访。MCI 定义为患者至少 18 个月未在诊所内或诊所外寻求护理,无论中断后是否返回护理。使用 Cox 模型评估 MCI 与 HIV 诊断和随访期间的社会人口统计学、临床和免疫病毒学特征之间的相关性。
MCI 的发生率为每 100 人年 2.5 例(95%置信区间 [CI] = 2.3-2.7)。在诊断后 6 个月以上开始治疗(风险比 [HR] = 1.30,95%CI = 1.10-1.54 与≤6 个月)或未报告初级保健医生(HR = 2.40;95%CI = 2.03-2.84)的患者中,MCI 更有可能发生。与出生在法国的患者相比,出生在撒哈拉以南非洲的患者(HR = 0.75,95%CI = 0.62-0.91)发生 MCI 的可能性较小。在随访期间,当最后一次 CD4 计数≤350 时(HR = 2.85,95%CI = 2.02-4.04 与>500 个细胞/mm3)和当患者未接受抗逆转录病毒治疗时(HR = 3.67,95%CI = 2.90-4.66),MCI 的风险增加。
在这家为大量移民提供服务的医院中,MCI 的发生率较低。就诊时 CD4 计数较低或未记录可能提示 MCI 的风险较高,尤其是在延迟接受 HIV 治疗或未报告初级保健医生的患者中。