GRAM 2.0, EA2656, UNICAEN, Normandie University Hospital, Caen, France.
Infectious Diseases Department, UNICAEN, Normandie University Hospital, Caen, France.
PLoS One. 2020 Oct 15;15(10):e0240417. doi: 10.1371/journal.pone.0240417. eCollection 2020.
The aim of our study was to identify HIV-positive patients at risk of medical care interruption (MCI) in a provincial city of a high-income country.
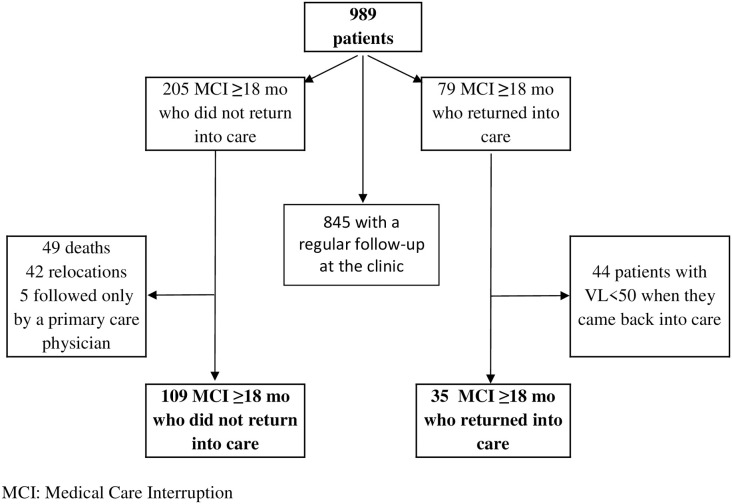
We estimated the incidence rate of MCI in 989 individuals followed in an HIV clinic in Caen University Hospital, Normandy, France, between January 2010 and May 2016. We enrolled patients over 18 years old who were seen at the clinic at least twice after HIV diagnosis. Patients were considered to be in MCI if they did not attend care in or outside the clinic for at least 18 months, regardless of whether or not they came back after interruption. We investigated sociodemographic, clinical and immunovirological characteristics at HIV diagnosis and during follow-up through a Cox model analysis.
The incidence rate of MCI was estimated to be 3.0 per 100 persons-years (95% confidence interval [CI] = 2.6-3.5). The independent risk factors for MCI were a linkage to care >6 months after HIV diagnosis (hazard ratio [HR] = 1.14; 95% CI = 1.08-1.21), a hepatitis C coinfection (HR = 1.76; 95% CI = 1.07-2.88), being born in Sub-Saharan Africa (HR = 2.18; 95% CI = 1.42-3.34 vs. in France) and not having a mailing address reported in the file (HR = 1.73; 95% CI = 1.07-2.80). During follow-up, the risk of MCI decreased when the patient was older (HR = 0.28; 95% CI = 0.15-0.51 when >45 vs. ≤ 30 years old) and increased when the patient was not on antiretroviral therapy (HR = 2.78; 95% CI = 1.66-4.63).
Our findings show that it is important to link HIV-positive individuals to care quickly after diagnosis and initiate antiretroviral therapy as soon as possible to retain them in care.
本研究旨在确定高收入国家某省会城市中面临医疗服务中断(MCI)风险的 HIV 阳性患者。
我们估计了 989 名在法国诺曼底卡昂大学医院 HIV 诊所接受随访的个体的 MCI 发生率,随访时间为 2010 年 1 月至 2016 年 5 月。我们纳入了在 HIV 诊断后至少两次在诊所就诊的年龄在 18 岁以上的患者。如果患者在诊所或诊所外至少 18 个月未接受治疗,无论中断后是否返回,我们均认为其处于 MCI 状态。我们通过 Cox 模型分析调查了 HIV 诊断时和随访期间的人口统计学、临床和免疫病毒学特征。
MCI 的发生率估计为每 100 人年 3.0 例(95%置信区间[CI] = 2.6-3.5)。MCI 的独立危险因素包括 HIV 诊断后 6 个月以上进行关联治疗(风险比[HR] = 1.14;95%CI = 1.08-1.21)、合并丙型肝炎感染(HR = 1.76;95%CI = 1.07-2.88)、出生于撒哈拉以南非洲地区(HR = 2.18;95%CI = 1.42-3.34 与出生于法国)和未在档案中报告邮寄地址(HR = 1.73;95%CI = 1.07-2.80)。在随访期间,当患者年龄较大时(当患者年龄大于 45 岁时,风险比为 0.28;95%CI = 0.15-0.51;与年龄小于等于 30 岁时相比),MCI 的风险降低,而当患者未接受抗逆转录病毒治疗时(风险比为 2.78;95%CI = 1.66-4.63),MCI 的风险增加。
我们的研究结果表明,重要的是在诊断后尽快将 HIV 阳性个体与医疗服务联系起来,并尽快启动抗逆转录病毒治疗,以确保他们继续接受治疗。