Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
Department of Preventive Medicine, Yonsei University College of Medicine, Seoul, Korea.
Diabetes Metab J. 2020 Apr;44(2):267-276. doi: 10.4093/dmj.2019.0001. Epub 2019 Feb 28.
Impaired diastolic heart function has been observed in persons with non-alcoholic fatty liver disease (NAFLD) and/or with type 2 diabetes mellitus (T2DM). However, it is unclear whether NAFLD fibrotic progression, i.e., non-alcoholic steatohepatitis, poses an independent risk for diastolic dysfunction in T2DM. We investigated the association between liver fibrosis and left ventricular (LV) diastolic dysfunction in T2DM.
We analyzed 606 patients with T2DM, aged ≥50 years, who had undergone liver ultrasonography and pulsed-wave Doppler echocardiography. Insulin sensitivity was measured by short insulin tolerance test. Presence of NAFLD and/or advanced liver fibrosis was determined by abdominal ultrasonography and NAFLD fibrosis score (NFS). LV diastolic dysfunction was defined according to transmitral peak early to late ventricular filling (E/A) ratio and deceleration time, using echocardiography.
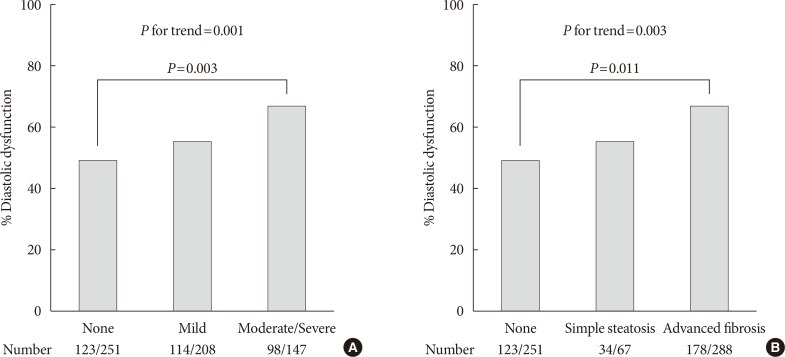
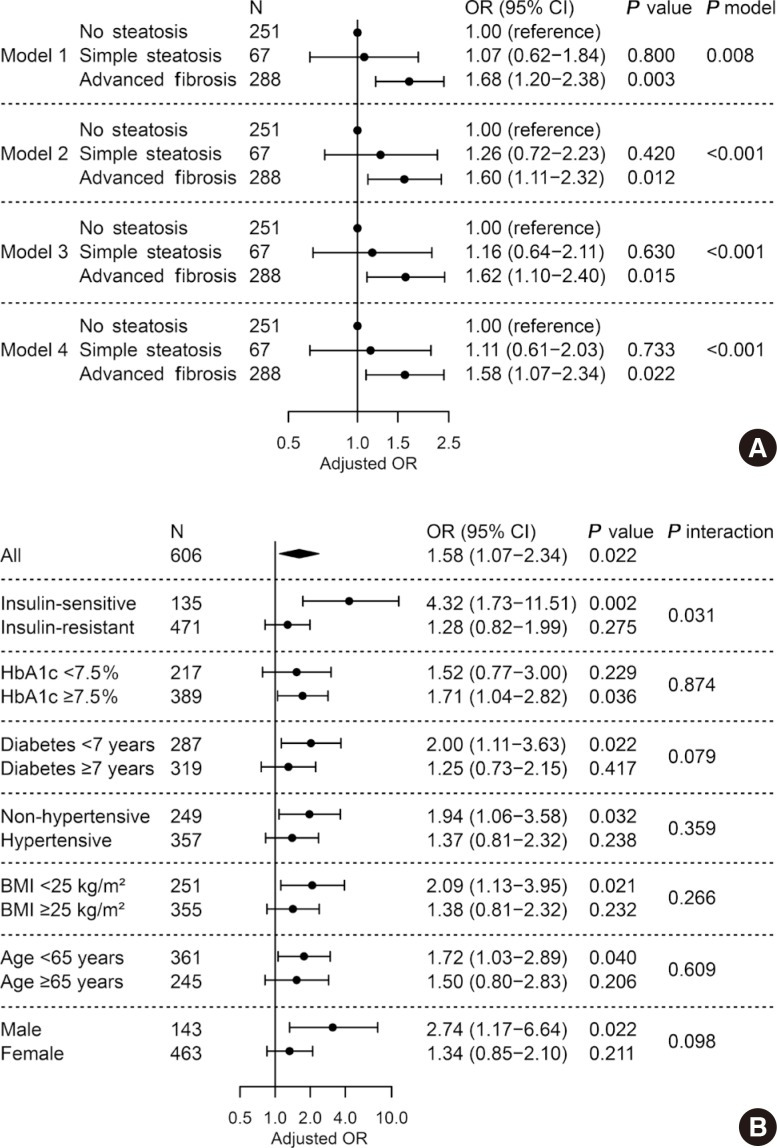
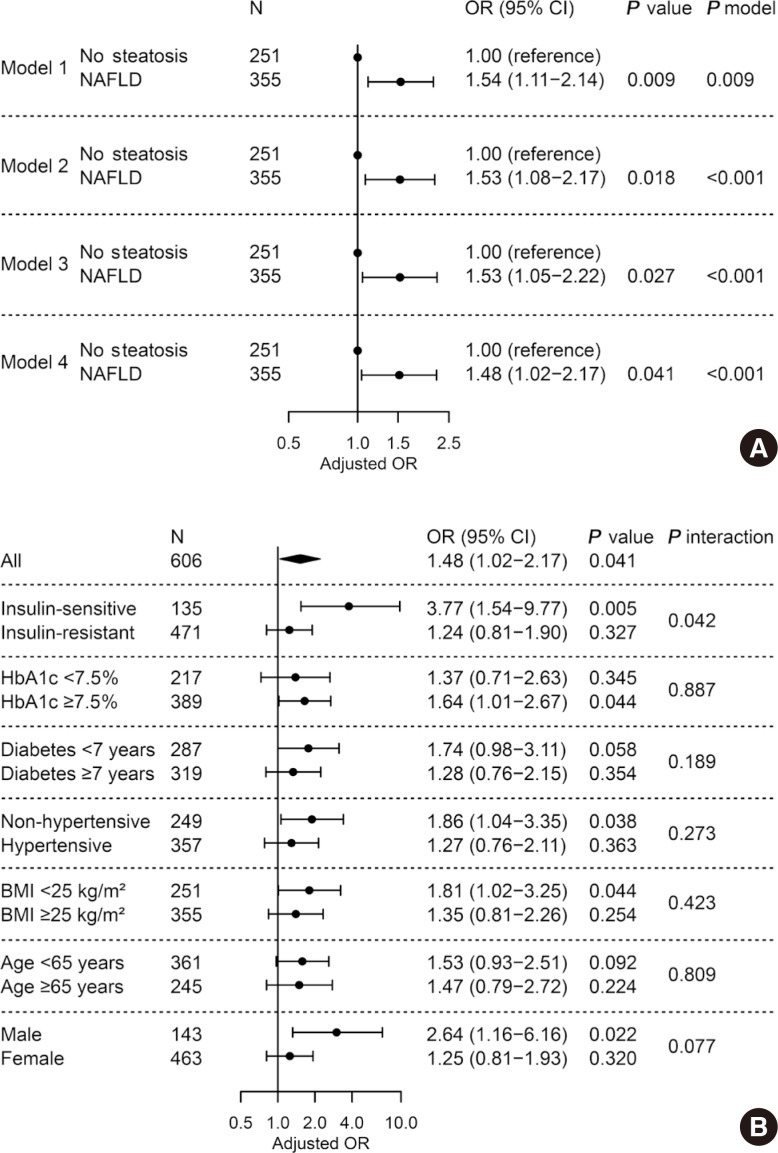
LV diastolic dysfunction was significantly more prevalent in the NAFLD versus non-NAFLD group (59.7% vs. 49.0%, =0.011). When NAFLD was stratified by NFS, subjects with advanced liver fibrosis exhibited a higher prevalence of diastolic dysfunction (49.0%, 50.7%, 61.8%; none, simple steatosis, advanced fibrosis, respectively; for trend=0.003). In multivariable logistic regression, liver fibrosis was independently associated with diastolic dysfunction (odds ratio [OR], 1.58; 95% confidence interval [CI], 1.07 to 2.34; =0.022) after adjusting for insulin resistance and cardiometabolic risk factors. This association remained significant in patients without insulin resistance (OR, 4.32; 95% CI, 1.73 to 11.51; =0.002).
Liver fibrosis was associated with LV diastolic dysfunction in patients with T2DM and may be an independent risk factor for diastolic dysfunction, especially in patients without systemic insulin resistance.
非酒精性脂肪性肝病(NAFLD)和/或 2 型糖尿病(T2DM)患者存在舒张功能障碍。然而,NAFLD 纤维化进展(即非酒精性肝炎)是否会增加 T2DM 患者舒张功能障碍的风险尚不清楚。我们研究了 T2DM 患者肝纤维化与左心室(LV)舒张功能障碍之间的关系。
我们分析了 606 例年龄≥50 岁的 T2DM 患者,这些患者均接受了肝脏超声和脉冲波多普勒超声心动图检查。胰岛素敏感性通过短胰岛素耐量试验来测量。NAFLD 和/或晚期肝纤维化的存在通过腹部超声和 NAFLD 纤维化评分(NFS)来确定。LV 舒张功能障碍根据超声心动图测量的二尖瓣峰早期到晚期心室充盈(E/A)比值和减速时间来定义。
与非 NAFLD 组相比,NAFLD 组 LV 舒张功能障碍更为常见(59.7%比 49.0%,=0.011)。当根据 NFS 将 NAFLD 分层时,肝纤维化程度较高的患者舒张功能障碍的发生率更高(分别为 49.0%、50.7%和 61.8%;无纤维化、单纯性脂肪变性、晚期纤维化,趋势检验=0.003)。在多变量逻辑回归中,在调整胰岛素抵抗和心血管代谢危险因素后,肝纤维化与舒张功能障碍独立相关(比值比 [OR],1.58;95%置信区间 [CI],1.07 至 2.34;=0.022)。在无胰岛素抵抗的患者中,这种相关性仍然显著(OR,4.32;95%CI,1.73 至 11.51;=0.002)。
在 T2DM 患者中,肝纤维化与 LV 舒张功能障碍相关,并且可能是舒张功能障碍的独立危险因素,尤其是在无系统性胰岛素抵抗的患者中。