Sasse Kent C, Gevorkian Jonathan, Lambin Rachel, Afshar Rami, Gardner Amy, Mehta Aradhana, Lambin John-Henry, Shinagawa Austin
K Sasse Surgical Associates, Reno, Nevada, USA.
Reno School of Medicine, University of Nevada, Reno, Nevada, USA.
JSLS. 2019 Jan-Mar;23(1). doi: 10.4293/JSLS.2018.00106.
There is no current consensus on the management of large hiatal hernias concomitant with performance of a sleeve gastrectomy procedure. Proposed solutions have included performing a modified Nissen fundoplication, performing cruroplasty alone, utilizing the Linx device, performing cruroplasty with reinforcement material, and avoiding the sleeve procedure altogether in favor of a bypass procedure in order to minimize gastroesophageal reflux. Urinary bladder matrix (UBM) represents a biologically derived material for use in hiatal hernia repair reinforcement with the potential to improve durability of repair without incurring the risks of other reinforcement materials.
This study reports the results of a retrospective chart review of 32 cases of large hiatal hernia repair utilizing both primary crural repair and UBM reinforcement concomitant with laparoscopic sleeve gastrectomy by a single surgeon. Hernia diameter averaged 6 cm (range 4-9 cm). After an average of 1 year followup, 30 patients were assessed for subjective symptoms of gastroesophageal reflux (GERD) using the Gastroesophageal Reflux Disease-Health Related Quality of Life (GERD-HRQL) score. Twenty patients were evaluated with either upper gastrointestinal (GI) series, endoscopy, or both.
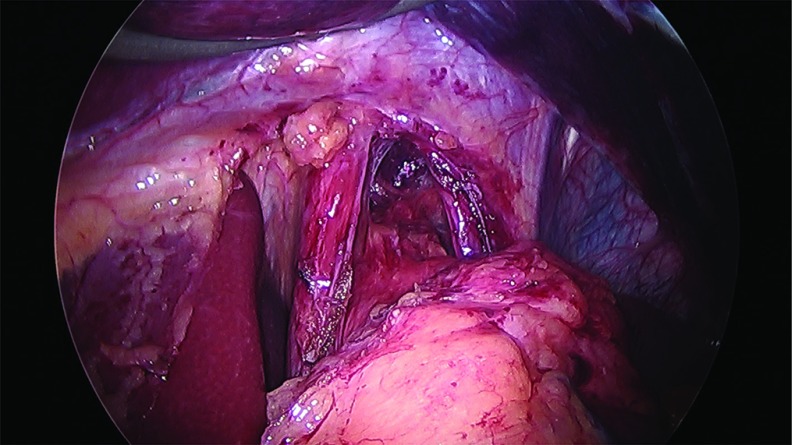
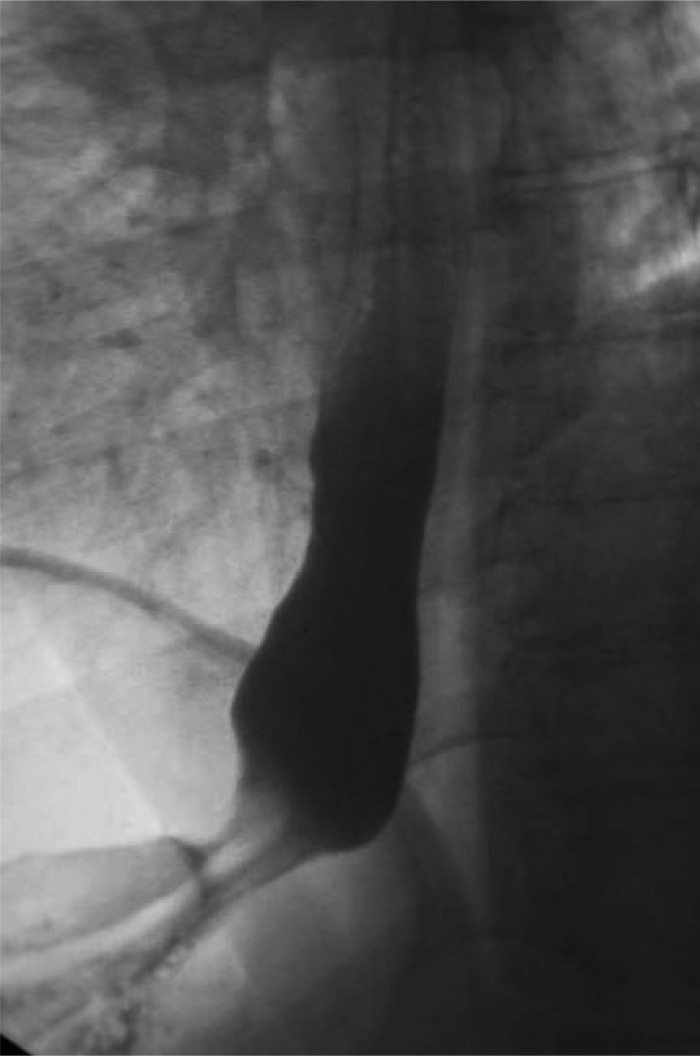
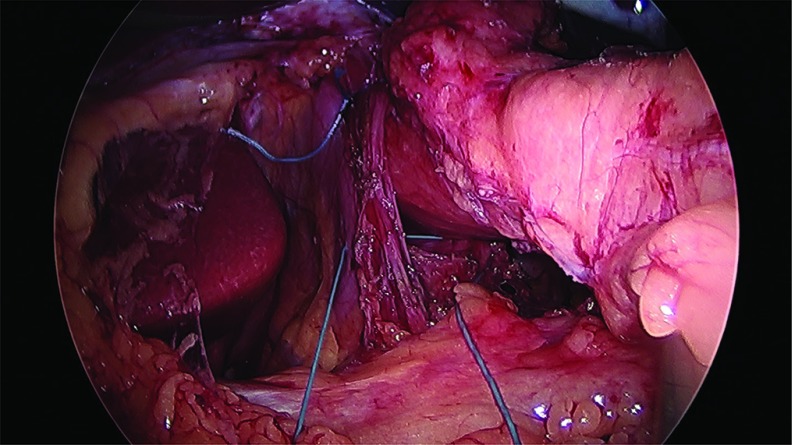
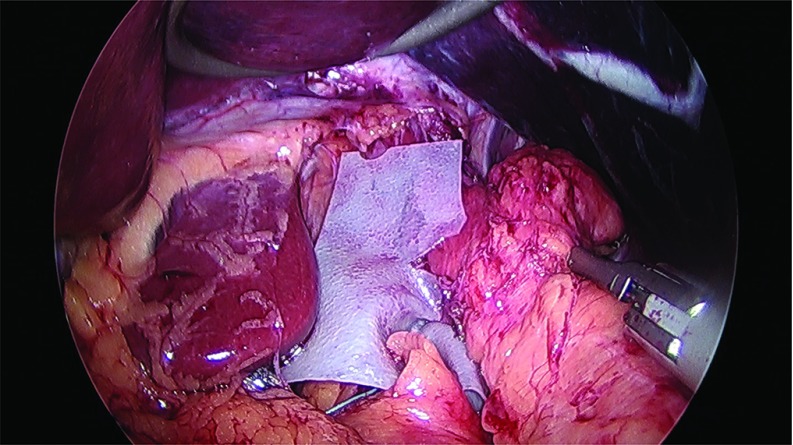
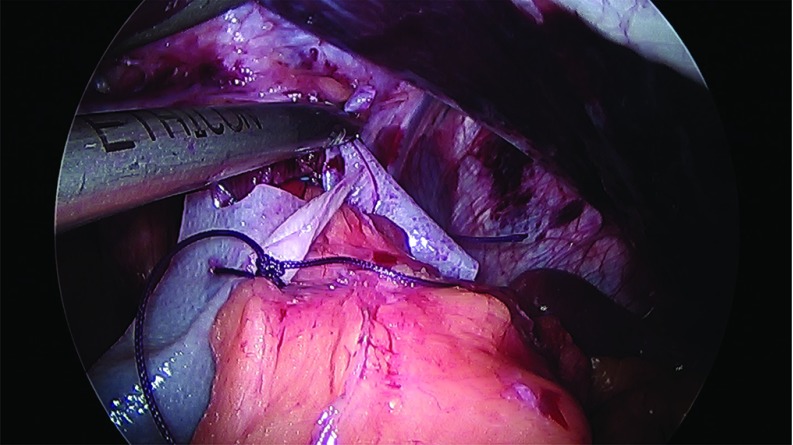
Each repair was successful and completed laparoscopically concomitant with sleeve gastrectomy. Anterior and posterior cruroplasty was performed using interrupted 0-Ethibond suture using the Endostitch device. The UBM graft exhibited favorable handling characteristics placed as a keyhole geometry sutured to the crura with absorbable suture. A careful chart review was undertaken to assess for complications. There have been no reoperations. After a median of 12 months (range, 4-27 months) of followup, an assessment of recurrences or long-term complications was completed. Median GERD-HRQL score was 6, with a range of 0 to 64 (of possible 75), indicating very low-level reflux symptomatology. Follow-up upper GI radiographs or endoscopy were obtained in 20 cases and show intact repairs.
In this series of 32 cases, laparoscopic cruroplasty with UBM graft reinforcement has been effective and durable at 12 months of followup. This technique may offer one satisfactory solution for large hiatal hernia repair concomitant with laparoscopic sleeve gastrectomy that may achieve a durable repair with low GERD symptoms.
目前对于大型食管裂孔疝合并袖状胃切除术的管理尚无共识。提出的解决方案包括进行改良的nissen胃底折叠术、单独进行膈肌脚成形术、使用Linx装置、使用加固材料进行膈肌脚成形术,以及完全避免袖状手术而选择旁路手术,以尽量减少胃食管反流。膀胱基质(UBM)是一种生物衍生材料,用于食管裂孔疝修补加固,有可能提高修补的耐久性,而不会产生其他加固材料的风险。
本研究报告了对32例大型食管裂孔疝修补术的回顾性病历审查结果,这些手术均由同一外科医生在腹腔镜袖状胃切除术的同时进行了初次膈肌脚修补和UBM加固。疝直径平均为6厘米(范围4 - 9厘米)。平均随访1年后,使用胃食管反流病-健康相关生活质量(GERD-HRQL)评分对30例患者的胃食管反流主观症状进行评估。20例患者接受了上消化道(GI)造影、内镜检查或两者检查。
每次修补均成功,并在腹腔镜下与袖状胃切除术同时完成。使用Endostitch装置,采用间断0号Ethibond缝线进行前后膈肌脚成形术。UBM移植物表现出良好的操作特性,以钥匙孔形状放置,并用可吸收缝线缝合到膈肌脚上。对病历进行了仔细审查以评估并发症。没有再次手术。在中位随访12个月(范围4 - 27个月)后,完成了对复发或长期并发症的评估。GERD-HRQL评分中位数为6,范围为0至64(可能的75分),表明反流症状非常轻微。20例患者进行了随访上消化道造影或内镜检查,显示修补完整。
在这32例病例系列中,腹腔镜下膈肌脚成形术联合UBM移植物加固在随访12个月时有效且持久。该技术可能为大型食管裂孔疝修补术联合腹腔镜袖状胃切除术提供一种令人满意的解决方案,该方案可能实现持久的修补且胃食管反流症状较轻。