Clinic of Neurology, Military Institute of Medicine, Warsaw, Poland,
Department of Radiology, Military Institute of Medicine, Warsaw, Poland.
Clin Interv Aging. 2019 Feb 27;14:493-503. doi: 10.2147/CIA.S195451. eCollection 2019.
The role of biomarkers in the prediction of acute ischemic stroke (AIS) outcome or response to thrombolytic therapy (with recombinant tissue plasminogen activator [rt-PA]) remains limited. The aim of this study was to evaluate whether mean platelet volume (MPV) could predict short-term functional outcome in patients with AIS following rt-PA treatment.
This was a retrospective analysis of 237 AIS patients (mean age 71.04±0.8 years, 50.6% women) consecutively admitted to a tertiary care center between 2011 and 2015.
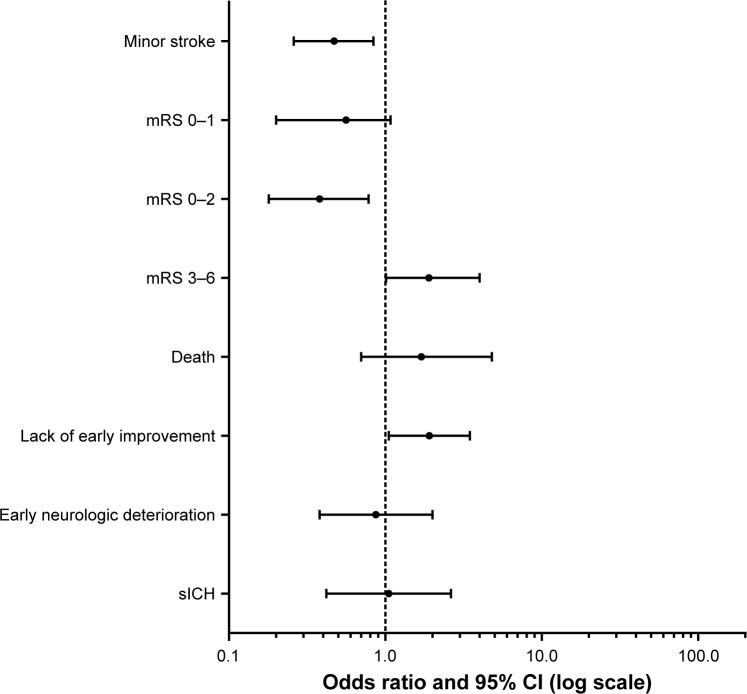
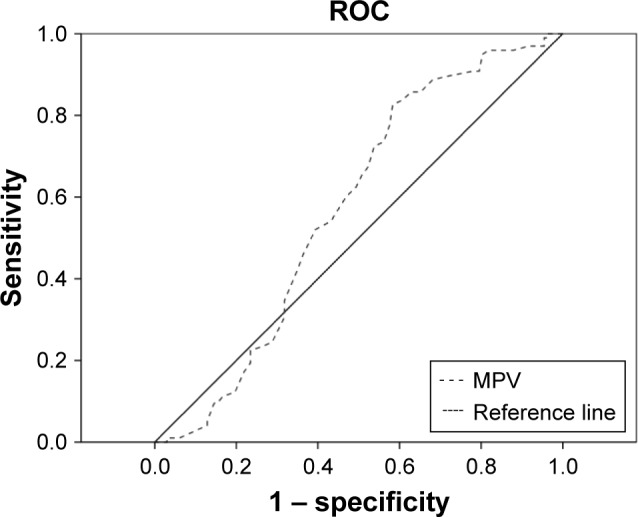
The mean MPV in the cohort was 9.8±0.35 fL (lowest tertile <7.29 fL, median 7.29-8.8 fL, and highest tertile >8.8 fL). Patients in the lowest tertile compared to median and highest tertiles were less often dependent (modified Rankin scale [mRS] ≥3) at admission (87.2% vs 96.1% and 96.1%, respectively, =0.04) and less often had a poor stroke outcome (mRS 4-6) at discharge (28.2% vs 55.3% and 44.7%, <0.01). However, there was no significant difference between tertiles with regard to AIS etiology, CT (Alberta Stroke Program Early CT) score, frequency of stroke due to large artery occlusion, risk of secondary hemorrhage, and early neurologic deterioration. Multivariable analysis after adjustment for confounders showed that patients in the second and third tertiles had a significantly higher risk of poor stroke outcome (OR =1.9, 95% CI =1.01-4), lack of early improvement (OR =1.91, 95% CI =1.05-3.47), lower chance of good outcome (mRS 0-2; OR =0.38, 95% CI =0.18-0.78), or minor stroke at discharge (OR =0.47, 95% CI =0.26-0.84). Receiver operating characteristic analysis for prediction of poor stroke outcome showed that the optimal cut-off point of MPV was 8.8 fL (area under the curve 0.586 [0.512-0.659], =0.03) with a sensitivity of 82.7% and a specificity of 43.9%.
Disabling or fatal ischemic stroke in thrombolyzed patients was observed more often in patients with high admission MPV. The prognostic value of MPV was independent of other well-defined individual risk factors.
生物标志物在预测急性缺血性脑卒中(AIS)结局或对溶栓治疗(重组组织型纤溶酶原激活剂 [rt-PA])的反应中的作用仍然有限。本研究旨在评估平均血小板体积(MPV)是否可以预测接受 rt-PA 治疗的 AIS 患者的短期功能结局。
这是对 2011 年至 2015 年连续入住三级护理中心的 237 名 AIS 患者(平均年龄 71.04±0.8 岁,50.6%为女性)的回顾性分析。
该队列中的平均 MPV 为 9.8±0.35 fL(最低三分位<7.29 fL,中位数 7.29-8.8 fL,最高三分位>8.8 fL)。与中位数和最高三分位相比,最低三分位的患者入院时依赖性(改良 Rankin 量表 [mRS]≥3)的发生率较低(87.2%、96.1%和 96.1%,=0.04),出院时卒中结局较差(mRS 4-6)的发生率也较低(28.2%、55.3%和 44.7%,<0.01)。然而,三分位之间在 AIS 病因、CT(阿尔伯塔卒中计划早期 CT)评分、大动脉闭塞所致卒中的频率、继发性出血风险和早期神经功能恶化方面无显著差异。调整混杂因素后的多变量分析显示,第二和第三三分位的患者卒中结局较差(OR=1.9,95%CI=1.01-4)、缺乏早期改善(OR=1.91,95%CI=1.05-3.47)、良好结局(mRS 0-2;OR=0.38,95%CI=0.18-0.78)或出院时轻度卒中(OR=0.47,95%CI=0.26-0.84)的可能性较低。预测不良卒中结局的受试者工作特征分析显示,MPV 的最佳截断值为 8.8 fL(曲线下面积 0.586 [0.512-0.659],=0.03),其敏感性为 82.7%,特异性为 43.9%。
接受溶栓治疗的患者中,高入院 MPV 与致残或致死性缺血性卒中的发生更相关。MPV 的预后价值独立于其他明确的个体危险因素。