Departments of Internal Medicine.
Biostatistics.
Clin J Am Soc Nephrol. 2019 Apr 5;14(4):567-575. doi: 10.2215/CJN.11010918. Epub 2019 Mar 19.
Cognitive impairment is common in patients with kidney disease and can affect physicians' perception and/or patients' ability to complete the pretransplant evaluation. We examined whether cognitive impairment influences the likelihood for transplant listing and whether patients with cognitive impairment take longer to be listed.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: We conducted a single-center longitudinal cohort study. Patients presenting for their index kidney transplant evaluation were screened for cognitive impairment using the Montreal Cognitive Assessment. A score <26 indicated cognitive impairment. The transplant selection committee was blinded to the scores. Kaplan-Meier analysis assessed time to active listing by level of cognition. A Cox proportional hazards model that included age, sex, race/ethnicity, smoking, coronary artery disease, and diabetes was constructed to evaluate the association between Montreal Cognitive Assessment score and listing for transplant.
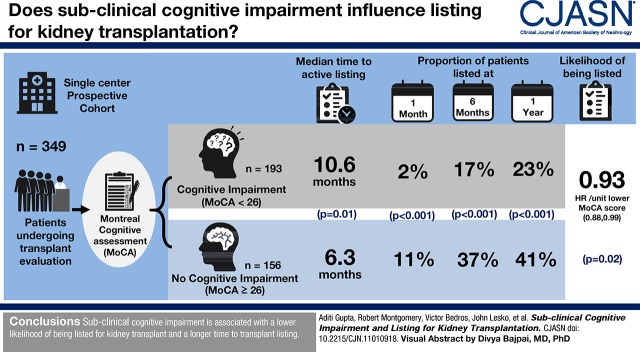
In total, 349 patients who underwent Montreal Cognitive Assessment testing at their initial visit were included in the analysis. Patients with cognitive impairment were more likely to be older, black, and smokers. The time to listing in patients with cognitive impairment was longer than the time to listing in those with no cognitive impairment (median time, 10.6 versus 6.3 months; log rank test =0.01). Cognitive impairment was independently associated with a lower likelihood of being listed for transplant (hazard ratio, 0.93 per unit lower Montreal Cognitive Assessment score; 95% confidence interval, 0.88 to 0.99; =0.02). A lower proportion of patients with cognitive impairment were listed compared with patients without cognitive impairment at 1 month (2% versus 11%), 6 months (17% versus 37%), and 1 year (23% versus 41%), (<0.001 for all).
Cognitive impairment is associated with a lower likelihood of being listed for kidney transplant, and is associated with longer time to transplant listing.
认知障碍在肾病患者中很常见,会影响医生的认知和/或患者完成移植前评估的能力。我们研究了认知障碍是否会影响患者被列入移植名单的可能性,以及认知障碍患者是否需要更长时间才能被列入名单。
设计、地点、参与者和测量:我们进行了一项单中心纵向队列研究。在进行指数肾移植评估时,对患者进行蒙特利尔认知评估以筛查认知障碍。得分<26 表示认知障碍。移植选择委员会对评分情况不知情。采用 Kaplan-Meier 分析评估认知水平与活跃名单之间的时间关系。构建 Cox 比例风险模型,纳入年龄、性别、种族/民族、吸烟、冠状动脉疾病和糖尿病,以评估蒙特利尔认知评估评分与移植名单之间的关联。
共有 349 名在首次就诊时接受蒙特利尔认知评估测试的患者纳入分析。认知障碍患者更可能年龄较大、为黑人且为吸烟者。认知障碍患者的列表时间长于无认知障碍患者(中位时间:10.6 个月比 6.3 个月;对数秩检验=0.01)。认知障碍与被列入移植名单的可能性较低独立相关(风险比,每降低 1 单位蒙特利尔认知评估得分降低 0.93;95%置信区间,0.88 至 0.99;=0.02)。与无认知障碍患者相比,认知障碍患者在 1 个月(2%比 11%)、6 个月(17%比 37%)和 1 年(23%比 41%)时被列入名单的比例较低(所有 P<0.001)。
认知障碍与被列入肾脏移植名单的可能性较低相关,且与移植名单时间较长相关。