Hematology, Hospital Universitario Puerta de Hierro-Majadahonda, Madrid
Hematology, Hospital Ramon y Cajal, Madrid.
Haematologica. 2019 Nov;104(11):2249-2257. doi: 10.3324/haematol.2018.204891. Epub 2019 Mar 19.
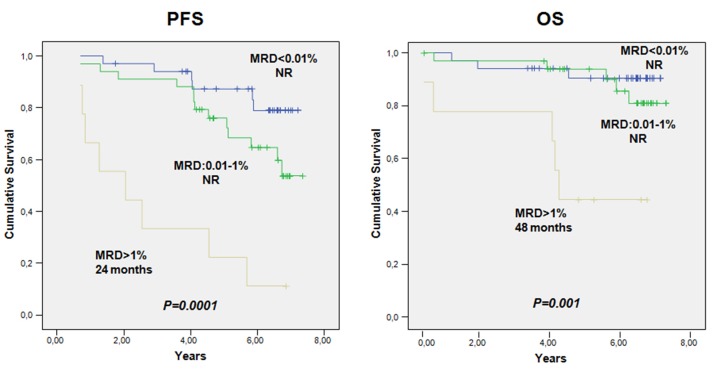
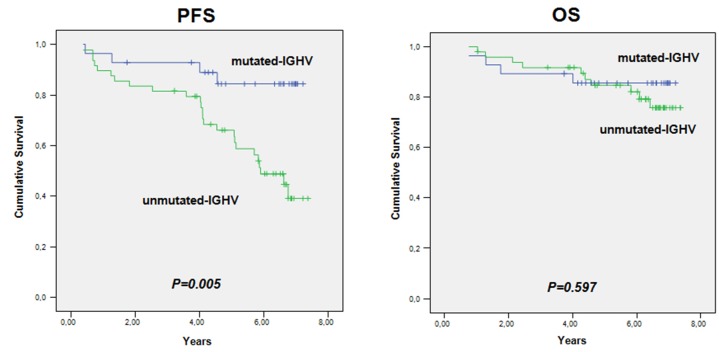
It has been postulated that monitoring measurable residual disease (MRD) could be used as a surrogate marker of progression-free survival (PFS) in chronic lymphocytic leukemia (CLL) patients after treatment with immunochemotherapy regimens. In this study, we analyzed the outcome of 84 patients at 3 years of follow-up after first-line treatment with fludarabine, cyclophosphamide and rituximab (FCR) induction followed by 36 months of rituximab maintenance thearpy. MRD was assessed by a quantitative four-color flow cytometry panel with a sensitivity level of 10 Eighty out of 84 evaluable patients (95.2%) achieved at least a partial response or better at the end of induction. After clinical evaluation, 74 patients went into rituximab maintenance and the primary endpoint was assessed in the final analysis at 3 years of follow-up. Bone marrow (BM) MRD analysis was performed after the last planned induction course and every 6 months in cases with detectable residual disease during the 36 months of maintenance therapy. Thirty-seven patients (44%) did not have detectable residual disease in the BM prior to maintenance therapy. Interestingly, 29 patients with detectable residual disease in the BM after induction no longer had detectable disease in the BM following maintenance therapy. After a median followup of 6.30 years, the median overall survival (OS) and PFS had not been reached in patients with either undetectable or detectable residual disease in the BM, who had achieved a complete response at the time of starting maintenance therapy. Interestingly, univariate analysis showed that after rituximab maintenance OS was not affected by IGHV status (mutated unmutated OS: 85.7% alive at 7.2 years 79.6% alive at 7.3 years, respectively). As per protocol, 15 patients (17.8%), who achieved a complete response and undetectable peripheral blood and BM residual disease after four courses of induction, were allowed to stop fludarabine and cyclophosphamide and complete two additional courses of rituximab and continue with maintenance therapy for 18 cycles. Surprisingly, the outcome in this population was similar to that observed in patients who received the full six cycles of the induction regimen. These data show that, compared to historic controls, patients treated with FCR followed by rituximab maintenance have high-quality responses with fewer relapses and improved OS. The tolerability of this regime is favorable. Furthermore, attaining an early undetectable residual disease status could shorten the duration of chemoimmunotherapy, reducing toxicities and preventing long-term side effects. The analysis of BM MRD after fludarabine-based induction could be a powerful predictor of post-maintenance outcomes in patients with CLL undergoing rituximab maintenance and could be a valuable tool to identify patients at high risk of relapse, influencing further treatment strategies. This trial is registered with EudraCT n. 2007-002733-36 and ClinicalTrials.gov Identifier: NCT00545714.
据推测,在接受免疫化学疗法治疗后,监测可测量的残留疾病 (MRD) 可以作为慢性淋巴细胞白血病 (CLL) 患者无进展生存期 (PFS) 的替代标志物。在这项研究中,我们分析了 84 例患者在接受氟达拉滨、环磷酰胺和利妥昔单抗 (FCR) 诱导治疗后 3 年的随访结果,随后进行了 36 个月的利妥昔单抗维持治疗。通过灵敏度为 10-8 的定量四色流式细胞术面板评估 MRD。84 例可评估患者中,80 例(95.2%)在诱导结束时至少达到部分缓解或更好的缓解。在临床评估后,74 例患者接受了利妥昔单抗维持治疗,主要终点在 3 年随访的最终分析中进行评估。在最后一次计划的诱导疗程后进行骨髓 (BM) MRD 分析,并在维持治疗的 36 个月期间,如果在残留疾病检测到残留疾病,则每 6 个月进行一次分析。在维持治疗前,37 例(44%)患者的 BM 中未检测到残留疾病。有趣的是,在诱导后 BM 中可检测到残留疾病的 29 例患者在维持治疗后不再可检测到 BM 中的疾病。中位随访 6.30 年后,在维持治疗时达到完全缓解且 BM 中未检测到残留疾病的患者的中位总生存期 (OS) 和 PFS 尚未达到。有趣的是,单因素分析表明,在接受利妥昔单抗维持治疗的患者中,OS 不受 IGHV 状态的影响(突变型 未突变型 OS:7.2 年时 85.7%存活 7.3 年时 79.6%存活)。根据方案,在接受 4 个疗程诱导后达到完全缓解且外周血和 BM 残留疾病不可检测的 15 例患者(17.8%)被允许停用氟达拉滨和环磷酰胺,并完成另外 2 个疗程的利妥昔单抗治疗,并继续进行 18 个周期的维持治疗。令人惊讶的是,该人群的结果与接受完整 6 个疗程诱导方案的患者观察到的结果相似。这些数据表明,与历史对照相比,接受 FCR 治疗后接受利妥昔单抗维持治疗的患者具有高质量的缓解,复发较少,OS 改善。该方案的耐受性良好。此外,早期达到不可检测的残留疾病状态可以缩短化疗免疫治疗的持续时间,降低毒性并预防长期副作用。在接受利妥昔单抗维持治疗的 CLL 患者中,在接受氟达拉滨为基础的诱导后分析 BM MRD 可以成为预测维持后结局的有力指标,并可能成为识别高复发风险患者的有价值工具,从而影响进一步的治疗策略。该试验在 EudraCT 注册 n. 2007-002733-36,并在 ClinicalTrials.gov 注册标识符:NCT00545714。