Division of Pulmonology and Critical Care Medicine, Department of Medicine, Sungkyunkwan University School of Medicine, Seoul, Korea.
Division of Pulmonary Medicine and Allergy, Department of Internal Medicine, Hanyang University, School of Medicine, Seoul, Korea.
Sci Rep. 2019 Mar 20;9(1):4941. doi: 10.1038/s41598-019-39671-8.
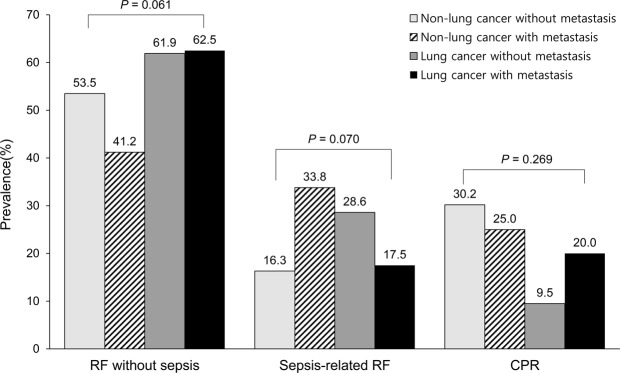
Few data are available regarding treatment outcomes in lung cancer patients with metastasis who initiated mechanical ventilation in the emergency department (ED). We aimed to evaluate 28-day mortality in lung cancer patients with metastasis who initiated mechanical ventilation in the ED. Patients with solid malignancy who initiated mechanical ventilation in the ED of a tertiary hospital were retrospectively identified and stratified into four groups according to the presence of lung cancer and metastasis. Among 212 included patients, the mortality rates by the 28 hospital day were as follows: 44.2% (19/43) in non-lung cancer patients without metastasis, 63.2% (43/68) in non-lung cancer patients with metastasis, 52.4% (11/21) in lung cancer patients without metastasis, and 66.2% (53/80) in lung cancer patients with metastasis. In multivariable analysis, lung cancer patients with metastasis had significantly higher odds ratio for 28-day mortality than non-lung cancer patients without metastasis (adjusted odds ratio [OR] = 7.17, 95% confidence interval [CI] = 2.14-24.01). Sepsis-related respiratory failure (adjusted OR = 2.60, 95% CI = 1.16-5.84) and cardiopulmonary resuscitation (adjusted OR = 13.34, 95% CI = 4.45-39.95) over respiratory failure without sepsis and acute organ dysfunction process measured by sequential organ failure assessment (SOFA) score (adjusted OR = 1.15, 95% CI = 1.05-12.6) were independently associated with an increase in mortality rate. In conclusion, the treatment outcomes in lung cancer patients with metastasis who initiated mechanical ventilation in the ED were poor. Aggressive resuscitation versus end-of-life care in advance of an unexpected medical crisis should be considered in lung cancer patients with metastasis via a multidisciplinary approach with a consideration of underlying comorbid illnesses in the acute organ dysfunction processes.
关于在急诊科(ED)开始机械通气的转移性肺癌患者的治疗结果,数据很少。我们旨在评估在 ED 开始机械通气的转移性肺癌患者的 28 天死亡率。在一家三级医院的 ED 接受机械通气的实体恶性肿瘤患者被回顾性识别,并根据是否存在肺癌和转移分为四组。在 212 名纳入患者中,28 天住院死亡率如下:无肺癌和无转移的非肺癌患者为 44.2%(19/43),无肺癌和有转移的非肺癌患者为 63.2%(43/68),无肺癌和无转移的肺癌患者为 52.4%(11/21),有肺癌和有转移的肺癌患者为 66.2%(53/80)。多变量分析显示,有转移的肺癌患者的 28 天死亡率的优势比明显高于无转移的非肺癌患者(调整后的优势比[OR] = 7.17,95%置信区间[CI] = 2.14-24.01)。与无败血症的呼吸衰竭相关的败血症相关性呼吸衰竭(调整后的 OR = 2.60,95%CI = 1.16-5.84)和心肺复苏(调整后的 OR = 13.34,95%CI = 4.45-39.95)以及通过序贯器官衰竭评估(SOFA)评分测量的急性器官功能障碍过程中无败血症和无呼吸衰竭(调整后的 OR = 1.15,95%CI = 1.05-12.6)与死亡率的增加独立相关。总之,在 ED 开始机械通气的转移性肺癌患者的治疗结果较差。通过多学科方法,在意外医疗危机之前,应考虑对转移性肺癌患者进行积极的复苏与生命终末期护理,并考虑急性器官功能障碍过程中的潜在合并症。