Orimoloye Olusola A, Kambhampati Swetha, Hicks Albert J, Al Rifai Mahmoud, Silverman Michael G, Whelton Seamus, Qureshi Waqas, Ehrman Jonathan K, Keteyian Steven J, Brawner Clinton A, Dardari Zeina, Al-Mallah Mouaz H, Blaha Michael J
Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, USA.
Department of Medicine, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Arch Med Sci. 2019 Mar;15(2):350-358. doi: 10.5114/aoms.2019.83290. Epub 2019 Mar 4.
Higher cardiorespiratory fitness (CRF) is associated with improved exercise capacity and quality of life in heart failure with preserved ejection fraction (HFpEF), but there are no large studies evaluating the association of HFpEF, CRF, and long-term survival. We therefore aimed to determine the association between CRF and all-cause mortality, in patients with HFpEF.
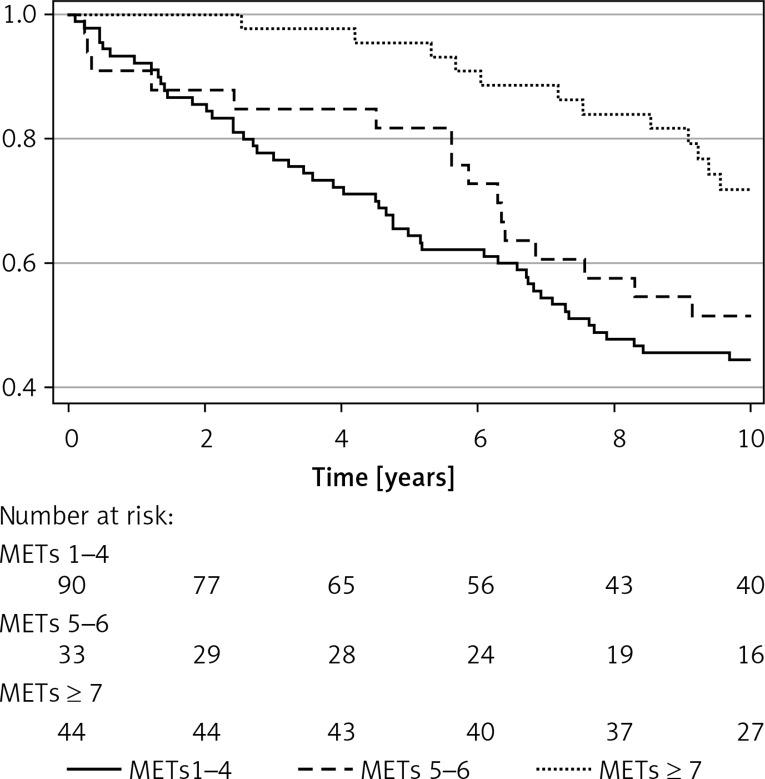
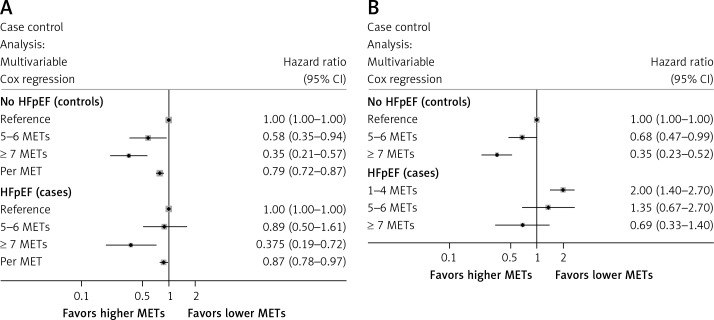
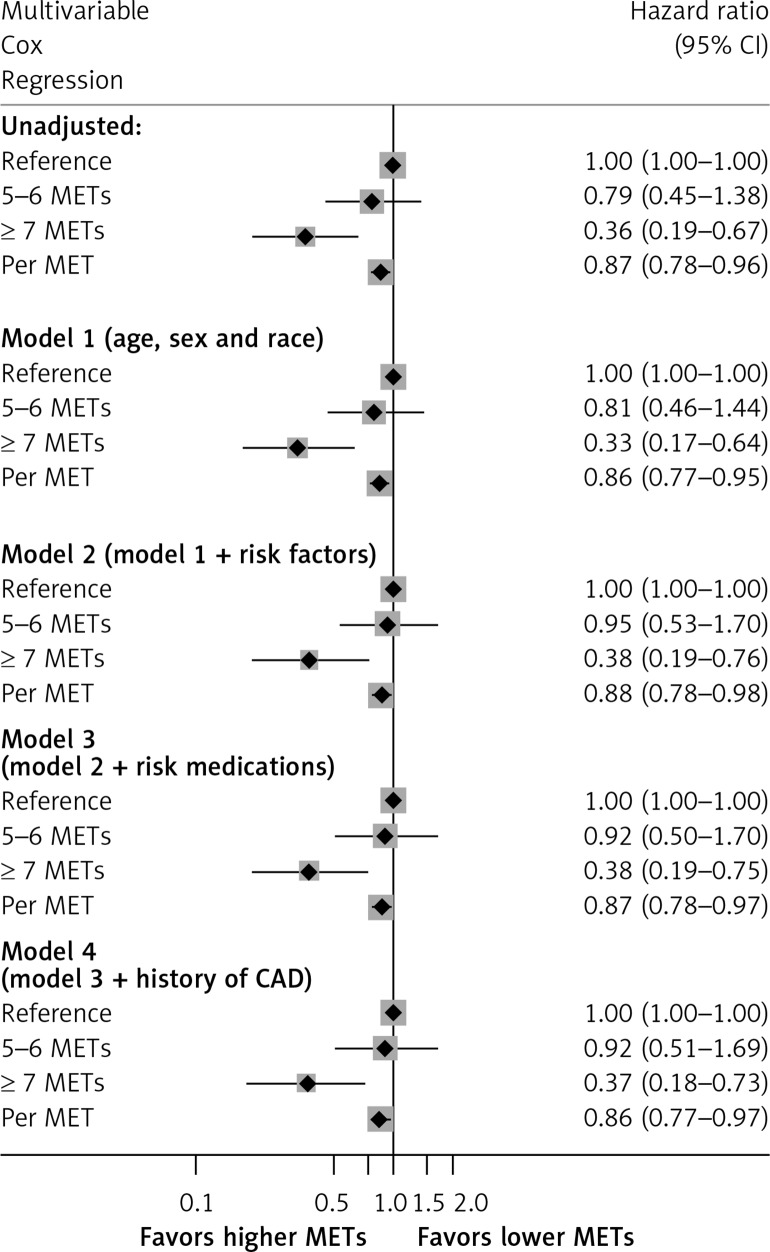
In the Henry Ford Exercise Testing (FIT) Project, 167 patients had baseline HFpEF, defined as a clinical diagnosis of heart failure with ejection fraction ≥ 50% on echocardiogram. The CRF was estimated from the peak workload (in METs) from a clinician-referred treadmill stress test and categorized as poor (1-4 METs), intermediate (5-6 METs), and moderate-high (≥ 7 METs). Additional analyses assessing the effect of HFpEF and CRF on mortality were also conducted, matching HFpEF patients to non-HFpEF patients using propensity scores.
Mean age was 64 ±13 years, with 55% women, and 46% Black. Over a median follow-up of 9.7 (5.2-18.9) years, there were 103 deaths. In fully adjusted models, moderate-high CRF was associated with 63% lower mortality risk (HR = 0.37, 95% CI: 0.18-0.73) compared to the poor-CRF group. In the propensity-matched cohort, HFpEF was associated with a HR of 2.3 (95% CI: 1.7-3.2) for mortality compared to non-HFpEF patients, which was attenuated to 1.8 (95% CI: 1.3-2.5) after adjusting for CRF.
Moderate-high CRF in patients with HFpEF is associated with improved survival, and differences in CRF partly explain the intrinsic risk of HFpEF. Randomized trials of interventions aimed at improving CRF in HFpEF are needed.
较高的心肺适能(CRF)与射血分数保留的心力衰竭(HFpEF)患者运动能力和生活质量的改善相关,但尚无大型研究评估HFpEF、CRF与长期生存之间的关联。因此,我们旨在确定HFpEF患者中CRF与全因死亡率之间的关联。
在亨利·福特运动测试(FIT)项目中,167例患者基线时患有HFpEF,定义为经超声心动图临床诊断为射血分数≥50%的心力衰竭。CRF通过临床医生推荐的跑步机压力测试的峰值工作量(以代谢当量计)估算,并分为差(1-4代谢当量)、中等(5-6代谢当量)和中高(≥7代谢当量)。还进行了其他分析,评估HFpEF和CRF对死亡率的影响,使用倾向评分将HFpEF患者与非HFpEF患者进行匹配。
平均年龄为64±13岁,55%为女性,46%为黑人。在中位随访9.7(5.2-18.9)年期间,有103例死亡。在完全调整模型中,与CRF差的组相比,中高CRF与死亡风险降低63%相关(HR=0.37,95%CI:0.18-0.73)。在倾向匹配队列中,与非HFpEF患者相比,HFpEF的死亡HR为2.3(95%CI:1.7-3.2),在调整CRF后降至1.8(95%CI:1.3-2.5)。
HFpEF患者的中高CRF与生存率提高相关,CRF的差异部分解释了HFpEF的内在风险。需要针对改善HFpEF患者CRF的干预措施进行随机试验。