Department of Emergency Medicine, Changhua Christian Hospital, Changhua, Taiwan.
School of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Crit Care. 2019 Mar 27;23(1):101. doi: 10.1186/s13054-019-2391-z.
The benefits of early epinephrine administration in pediatric with nontraumatic out-of-hospital cardiac arrest (OHCA) have been reported; however, the effects in pediatric cases of traumatic OHCA are unclear. Since the volume-related pharmacokinetics of early epinephrine may differ obviously with and without hemorrhagic shock (HS), beneficial or harmful effects of nonselective epinephrine stimulation (alpha and beta agonists) may also be enhanced with early administration. In this study, we aimed to analyze the therapeutic effect of early epinephrine administration in pediatric cases of HS and non-HS traumatic OHCA.
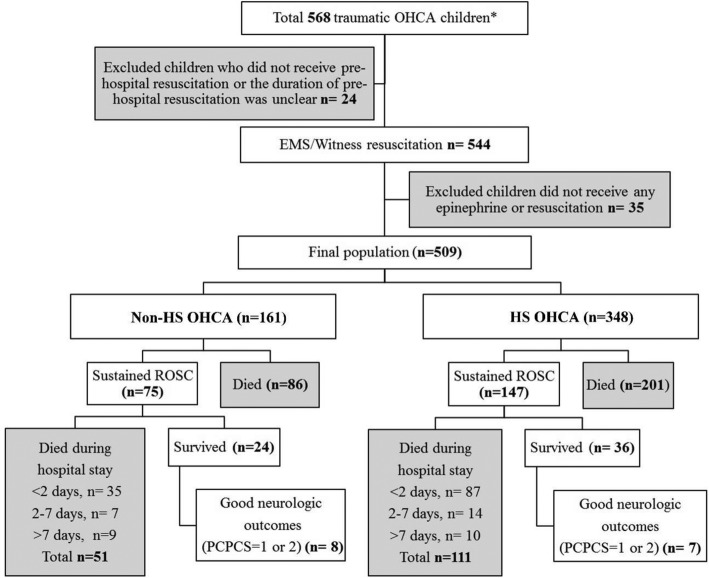
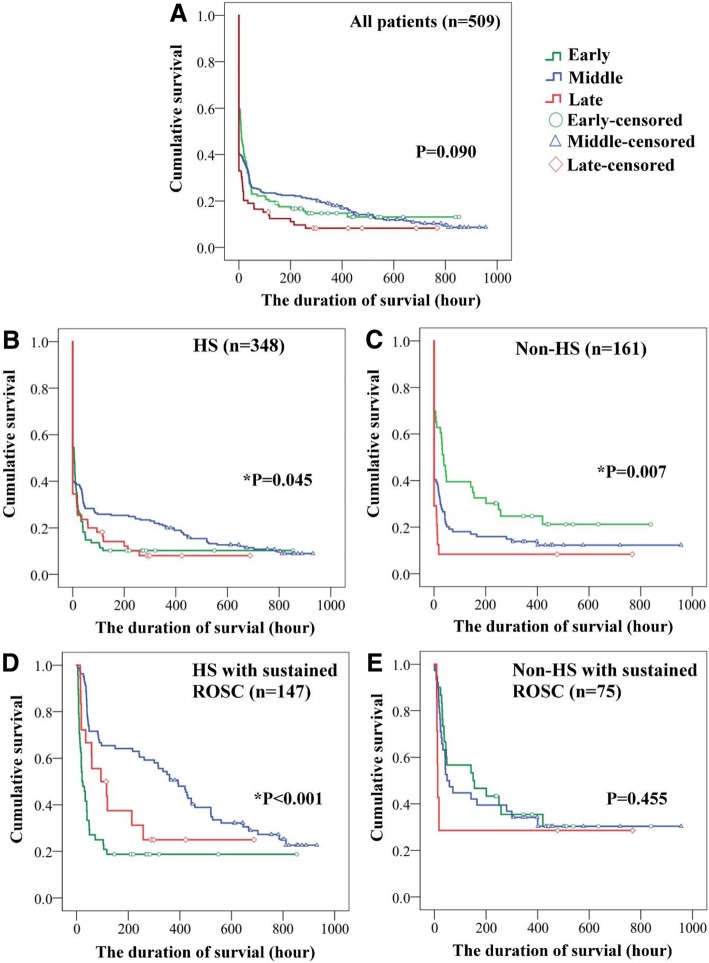
This was a multicenter retrospective study (2003-2014). Children (aged ≤ 19 years) who experienced traumatic OHCA and were administered epinephrine for resuscitation were included. Children were classified into the HS (blood loss > 30% of total body fluid) and non-HS groups. The demographics, outcomes, postresuscitation hemodynamics (the first hour) after the sustained return of spontaneous circulation (ROSC), and survival durations were analyzed and correlated with the time to epinephrine administration (early < 15, middle 15-30, late > 30 min) in the HS and non-HS groups. Cox regression analysis was used to adjust for risk factors of mortality.
A total of 509 children were included. Most of them (n = 348, 68.4%) had HS OHCA. Early epinephrine administration was implemented in 131 (25.7%) children. In both the HS and non-HS groups, early epinephrine administration was associated with achieving sustained ROSC (both p < 0.05) but was not related to survival or good neurological outcomes (without adjusting for confounding factors). However, early epinephrine administration in the HS group increased cardiac output but induced metabolic acidosis and decreased urine output during the initial postresuscitation period (all p < 0.05). After adjusting for confounding factors, early epinephrine administration was a risk factor of mortality in the HS group (HR 4.52, 95% CI 2.73-15.91).
Early epinephrine was significantly associated with achieving sustained ROSC in pediatric cases of HS and non-HS traumatic OHCA. For children with HS, early epinephrine administration was associated with both beneficial (increased cardiac output) and harmful effects (decreased urine output and metabolic acidosis) during the postresuscitation period. More importantly, early epinephrine was a risk factor associated with mortality in the HS group.
已报道早期肾上腺素给药对非创伤性院外心脏骤停(OHCA)儿童有益;然而,创伤性 OHCA 儿童的效果尚不清楚。由于早期肾上腺素给药的容量相关药代动力学在伴有和不伴有出血性休克(HS)时可能明显不同,非选择性肾上腺素刺激(α和β激动剂)的有益或有害作用也可能因早期给药而增强。在这项研究中,我们旨在分析早期肾上腺素给药对伴有和不伴有 HS 的创伤性 OHCA 儿童的治疗效果。
这是一项多中心回顾性研究(2003-2014 年)。纳入经历创伤性 OHCA 并接受肾上腺素复苏的儿童(年龄≤19 岁)。将儿童分为 HS(失血量>总体液的 30%)和非 HS 组。分析了两组的人口统计学、结局、自主循环恢复(ROSC)持续后 1 小时的复苏后血液动力学(早期 < 15 分钟、中期 15-30 分钟、晚期 > 30 分钟),并与 HS 和非 HS 组中肾上腺素给药时间(早期 < 15 分钟、中期 15-30 分钟、晚期 > 30 分钟)相关。Cox 回归分析用于调整死亡率的危险因素。
共纳入 509 名儿童。其中大多数(n=348,68.4%)患有 HS OHCA。早期肾上腺素给药在 131 名儿童(25.7%)中实施。在 HS 和非 HS 组中,早期肾上腺素给药均与实现持续 ROSC 相关(均 p<0.05),但与生存或良好的神经功能结局无关(未调整混杂因素)。然而,HS 组中早期肾上腺素给药在复苏后早期增加心输出量,但引起代谢性酸中毒和尿量减少(均 p<0.05)。在调整混杂因素后,早期肾上腺素给药是 HS 组死亡的危险因素(HR 4.52,95%CI 2.73-15.91)。
早期肾上腺素与 HS 和非 HS 创伤性 OHCA 儿童实现持续 ROSC 显著相关。对于 HS 儿童,早期肾上腺素给药在复苏后期间既有有益作用(增加心输出量),也有有害作用(尿量减少和代谢性酸中毒)。更重要的是,早期肾上腺素是 HS 组与死亡率相关的危险因素。