Department of Breast Surgery, The Royal Marsden NHS Foundation Trust, Downs Road, Sutton, Surrey, SM2 5PT, UK.
Department of Cancer Studies, Clinical Sciences Building, University of Leicester, Leicester, LE2 2LX, UK.
Br J Cancer. 2019 Apr;120(9):883-895. doi: 10.1038/s41416-019-0438-1. Epub 2019 Mar 29.
Immediate breast reconstruction (IBR) is routinely offered to improve quality-of-life for women requiring mastectomy, but there are concerns that more complex surgery may delay adjuvant oncological treatments and compromise long-term outcomes. High-quality evidence is lacking. The iBRA-2 study aimed to investigate the impact of IBR on time to adjuvant therapy.
Consecutive women undergoing mastectomy ± IBR for breast cancer July-December, 2016 were included. Patient demographics, operative, oncological and complication data were collected. Time from last definitive cancer surgery to first adjuvant treatment for patients undergoing mastectomy ± IBR were compared and risk factors associated with delays explored.
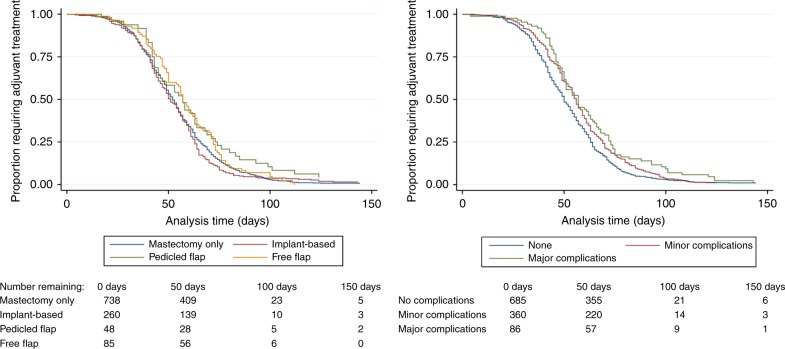
A total of 2540 patients were recruited from 76 centres; 1008 (39.7%) underwent IBR (implant-only [n = 675, 26.6%]; pedicled flaps [n = 105,4.1%] and free-flaps [n = 228, 8.9%]). Complications requiring re-admission or re-operation were significantly more common in patients undergoing IBR than those receiving mastectomy. Adjuvant chemotherapy or radiotherapy was required by 1235 (48.6%) patients. No clinically significant differences were seen in time to adjuvant therapy between patient groups but major complications irrespective of surgery received were significantly associated with treatment delays.
IBR does not result in clinically significant delays to adjuvant therapy, but post-operative complications are associated with treatment delays. Strategies to minimise complications, including careful patient selection, are required to improve outcomes for patients.
即刻乳房重建(IBR)通常被用于改善需要接受乳房切除术的女性的生活质量,但人们担心更复杂的手术可能会延迟辅助肿瘤治疗并影响长期预后。目前缺乏高质量的证据。iBRA-2 研究旨在调查 IBR 对辅助治疗时间的影响。
连续纳入 2016 年 7 月至 12 月期间因乳腺癌接受乳房切除术±IBR 的女性患者。收集患者的人口统计学、手术、肿瘤学和并发症数据。比较接受乳房切除术±IBR 的患者从最后一次确定性癌症手术到首次辅助治疗的时间,并探讨与延迟相关的风险因素。
共从 76 个中心招募了 2540 例患者;1008 例(39.7%)接受了 IBR(单纯植入物[n=675,26.6%];带蒂皮瓣[n=105,4.1%]和游离皮瓣[n=228,8.9%])。接受 IBR 的患者比接受乳房切除术的患者更常见需要再次入院或再次手术的并发症。需要辅助化疗或放疗的患者有 1235 例(48.6%)。两组患者的辅助治疗时间无显著差异,但无论手术与否,主要并发症与治疗延迟显著相关。
IBR 不会导致辅助治疗的临床显著延迟,但术后并发症与治疗延迟相关。需要采取策略来减少并发症,包括仔细选择患者,以改善患者的结局。