Division of Digestive and Liver Diseases, Department of Medicine, Cedars Sinai Medical Center, Los Angeles, CA, USA.
Comprehensive Transplant Center, Cedars Sinai Medical Center, Los Angeles, CA, USA.
Clin Mol Hepatol. 2019 Dec;25(4):335-343. doi: 10.3350/cmh.2019.0010. Epub 2019 Mar 29.
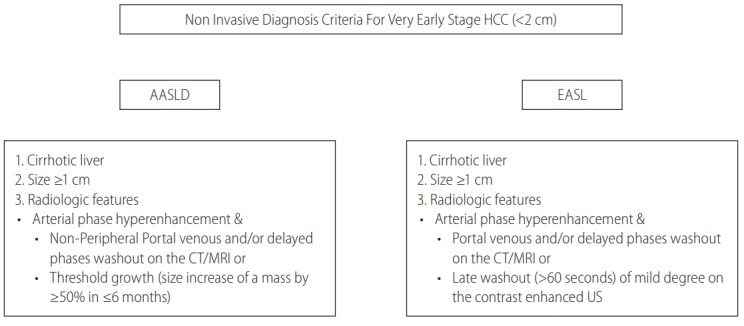
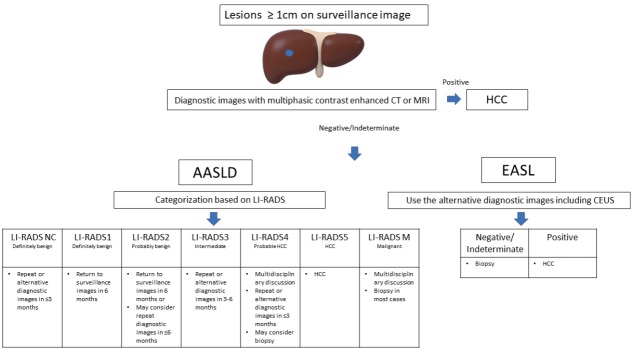
Very early stage hepatocellular carcinoma (HCC) is defined as a single tumor with the largest diameter of the lesion measuring 2 cm or less according to Barcelona Liver Cancer staging system. Detection of very early stage HCC is clinically important as it confers an excellent prognosis with the 5-year survival rates over 60 to 80% after patients receive curative treatments. While diagnosing HCC at a very early stage is crucial, it is technically challenging and may come with the physical or psychosocial harms related to diagnostic tests. It is further complicated by the fact that patients with very early stage HCC are not prioritized for liver transplant (LT) in the United States organ allocation system. When LT-eligible patients present with an indeterminate lesion measuring between 1 and 2 cm on the multiphasic computed tomography or magnetic resonance imaging, clinicians often observe patients carefully until the lesion grows up to 2 cm so that patients can be eligible to receive a Model for End-Stage Liver Disease (MELD) exception score for HCC in the United States. The European guideline recommends a routine biopsy of such lesion. In conclusion, attempting to detect very early stage HCC is difficult to achieve and controversial. Clinicians should take into account of the risk and the benefit of diagnostic tests, LT candidacy of patients and the local organ allocation system.
非常早期的肝细胞癌(HCC)定义为根据巴塞罗那肝癌分期系统,病变最大直径为 2 厘米或更小的单个肿瘤。非常早期 HCC 的检测在临床上很重要,因为它为患者接受根治性治疗后提供了超过 60%至 80%的 5 年生存率。虽然在非常早期诊断 HCC 非常重要,但这在技术上具有挑战性,并且可能会因诊断测试而带来身体或心理社会伤害。更为复杂的是,美国器官分配系统中,非常早期 HCC 患者没有被优先考虑进行肝移植(LT)。当 LT 合格的患者在多期 CT 或磁共振成像上出现 1 至 2 厘米之间的不确定病变时,临床医生通常会仔细观察患者,直到病变增大到 2 厘米,以便患者有资格在美国获得 HCC 的终末期肝病模型(MELD)例外评分。欧洲指南建议对这种病变进行常规活检。总之,试图检测非常早期的 HCC 是困难的,也是有争议的。临床医生应考虑诊断测试的风险和获益、患者的 LT 资格和当地的器官分配系统。