Department of Surgery, Herlev Hospital, University of Copenhagen, Herlev Ringvej 75, 2730, Herlev, Denmark.
Department of Surgery, Roskilde Hospital, University of Copenhagen, Sygehusvej 10, 4000, Roskilde, Denmark.
World J Surg Oncol. 2019 Apr 2;17(1):62. doi: 10.1186/s12957-019-1604-x.
It has been suggested that apart from tumour and nodal status, a range of patient-related and histopathological factors including lymph node yield and tumour location seems to have prognostic implications in stage I-III colon cancer. We analysed the prognostic implication of lymph node yield and tumour subsite in stage I-III colon cancer.
Data on patients with stage I to III adenocarcinoma of the colon and treated by curative resection in the period from 2003 to 2011 were extracted from the Danish Colorectal Cancer Group database, merged with information from the Danish National Patient Register and analysed.
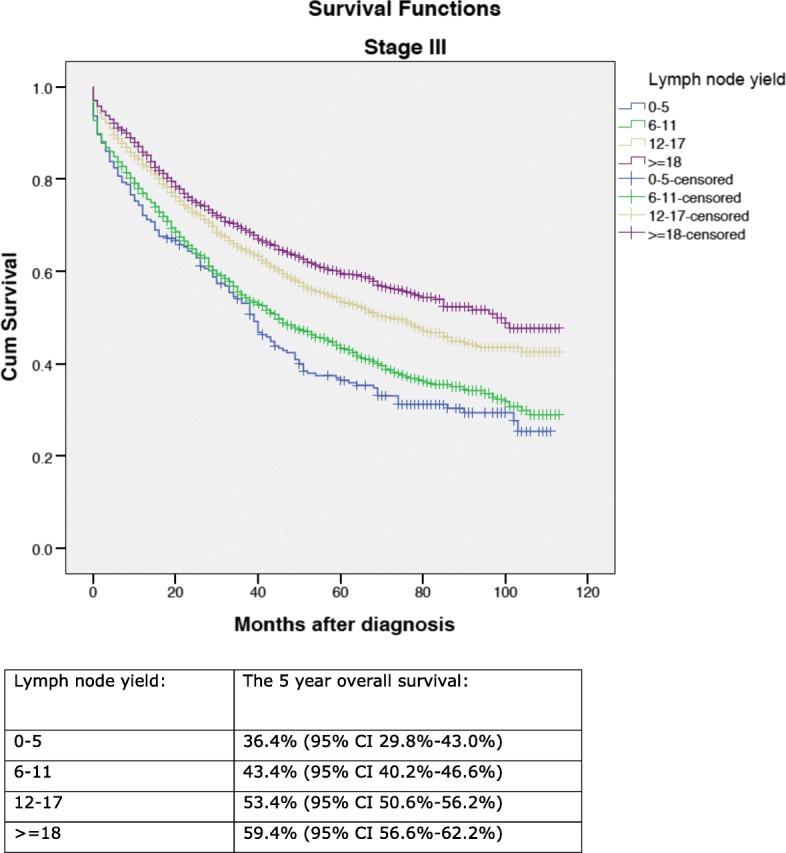
A total of 13,766 patients were included in the analysis. The 5-year overall survival ranged from 59.3% (95% CI 55.7-62.9%) (lymph node yield 0-5) to 74.0% (95% CI 71.8-76.2%) (lymph node yield ≥ 18) for patients with stage I-II disease (p < 0.0001) and from 36.4% (95% CI 29.8-43.0%) (lymph node yield 0-5) to 59.4% (95% CI 56.6-62.2%) (lymph node yield ≥ 18) for patients with stage III disease (p < 0.0001). The 5-year overall survival for tumour side left/right was 59.3% (95% CI 57.9-60.7%)/64.8% (CI 63.4-66.2%) (p < 0.0001). In the seven colonic tumour subsites, the 5-year overall survival ranged from 56.6% (95% CI 51.8-61.4%) at splenic flexure to 65.8% (95% CI 64.5-67.2%) in the sigmoid colon (p < 0.0001). In a cox regression analysis, lymph node yield and tumour side right/left were found to be prognostic factors. Tumours at the hepatic and splenic flexures had an adverse prognostic outcome.
For stage I-III colon cancer, a lymph node yield beyond the recommended 12 lymph nodes was associated with improved survival. Both subsite in the right colon, as well as subsite in the left colon, turned out with adverse prognostic outcome questioning a simple classification into right-sided and left-sided colon cancer.
除了肿瘤和淋巴结状态外,一系列与患者相关和组织病理学因素,包括淋巴结检出量和肿瘤部位,似乎对 I-III 期结肠癌具有预后意义。我们分析了淋巴结检出量和肿瘤部位在 I-III 期结肠癌中的预后意义。
从丹麦结直肠癌组数据库中提取了 2003 年至 2011 年期间接受根治性切除术治疗的 I 期至 III 期结肠癌患者的数据,并与丹麦国家患者登记处的信息合并进行分析。
共纳入 13766 例患者。I-II 期疾病患者的 5 年总生存率范围为 59.3%(95%CI 55.7-62.9%)(淋巴结检出量 0-5)至 74.0%(95%CI 71.8-76.2%)(淋巴结检出量≥18)(p<0.0001),而 III 期疾病患者的 5 年总生存率范围为 36.4%(95%CI 29.8-43.0%)(淋巴结检出量 0-5)至 59.4%(95%CI 56.6-62.2%)(淋巴结检出量≥18)(p<0.0001)。肿瘤侧左/右侧的 5 年总生存率分别为 59.3%(95%CI 57.9-60.7%)/64.8%(CI 63.4-66.2%)(p<0.0001)。在七个结肠肿瘤部位中,5 年总生存率范围从脾曲的 56.6%(95%CI 51.8-61.4%)到乙状结肠的 65.8%(95%CI 64.5-67.2%)(p<0.0001)。在 Cox 回归分析中,发现淋巴结检出量和肿瘤右侧/左侧是预后因素。肝曲和脾曲的肿瘤预后不良。
对于 I-III 期结肠癌,淋巴结检出量超过推荐的 12 枚与生存改善相关。右半结肠和左半结肠的部位均预后不良,质疑简单地将结肠癌分为右半结肠癌和左半结肠癌的分类方法。