Carstam Louise, Smits Anja, Milos Peter, Corell Alba, Henriksson Roger, Bartek Jiri, Jakola Asgeir Store
Department of Neurosurgery, Sahlgrenska University Hospital, Gothenburg, Sweden.
Institute of Neuroscience and Physiology, University of Gothenburg, Sahlgrenska Academy, Sweden.
Neurooncol Pract. 2019 Mar;6(2):124-133. doi: 10.1093/nop/npy023. Epub 2018 Jul 17.
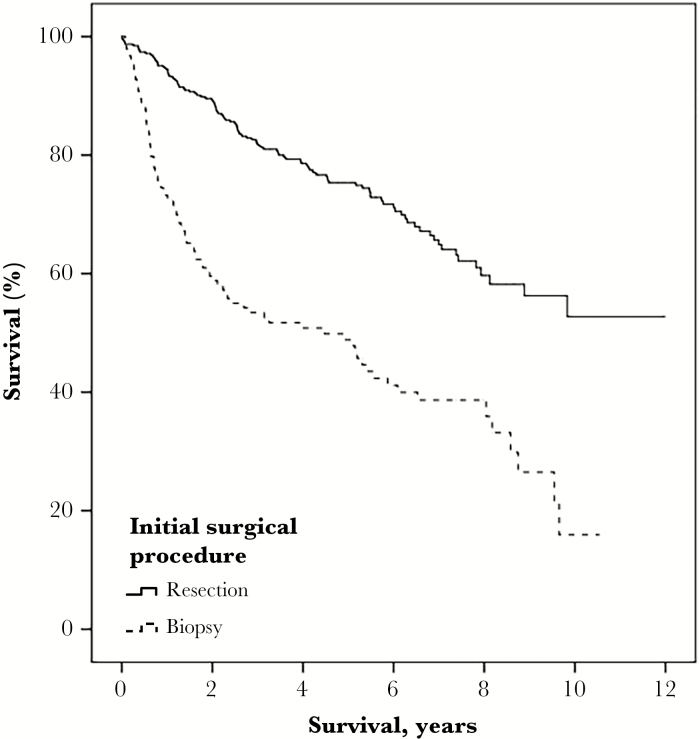
In the last decade, increasing evidence has evolved for early and maximal safe resection of diffuse low-grade gliomas (LGGs) regarding survival. However, changes in clinical practice are known to occur slowly and we do not know if the scientific evidence has yet resulted in changes in neurosurgical patterns of care.
The Swedish Brain Tumor Registry was used to identify all patients with a first-time histopathological diagnosis of LGG between 2005 and 2015. For analysis of surgical treatment patterns, we subdivided assessed time periods into 2005-2008, 2009-2012, and 2013-2015. Population-based data on patient and disease characteristics, surgical management, and outcomes were extracted.
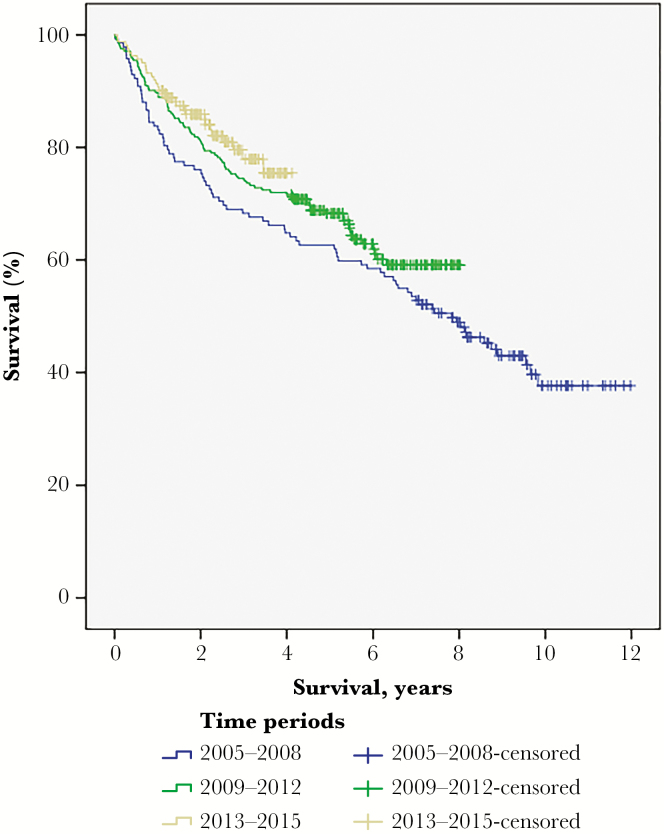
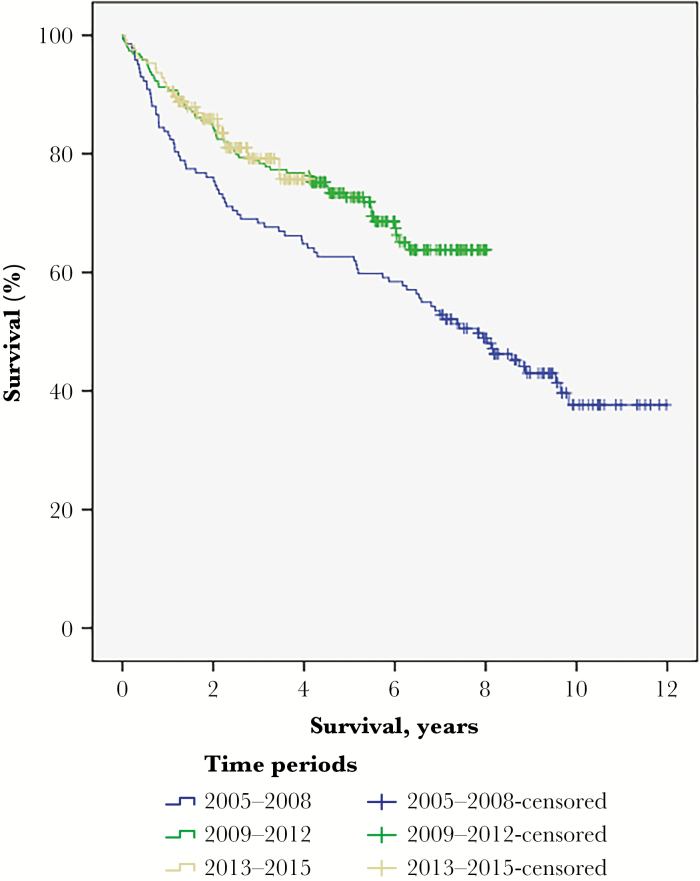
A total of 548 patients with diffuse World Health Organization grade II gliomas were identified: 142 diagnosed during 2005-2008, 244 during 2009-2012, and 162 during 2013-2015. Resection as opposed to biopsy was performed in 64.3% during 2005-2008, 74.2% during 2009-2012, and 74.1% during 2013-2015 ( = .08). There was no difference among the 3 periods regarding overall survival ( = .11). However, post hoc analysis of data from the 4 (out of 6) centers that covered all 3 time periods demonstrated a resection rate of 64.3% during 2005-2008, 77.4% during 2009-2012, and 75.4% during 2013-2015 ( = .02) and longer survival of patients diagnosed 2009 and onward ( = .04).
In this nationwide, population-based study we observed a shift over time in favor of LGG resection. Further, a positive correlation between the more active surgical strategy and longer survival is shown, although no causality can be claimed because of possible confounding factors.
在过去十年中,越来越多的证据表明,对于弥漫性低级别胶质瘤(LGG)患者,早期进行最大程度的安全切除可提高生存率。然而,临床实践的改变通常较为缓慢,我们尚不清楚科学证据是否已导致神经外科治疗模式发生变化。
利用瑞典脑肿瘤登记处的数据,确定了2005年至2015年间首次经组织病理学诊断为LGG的所有患者。为分析手术治疗模式,我们将评估时间段细分为2005 - 2008年、2009 - 2012年和2013 - 2015年。提取了基于人群的患者和疾病特征、手术管理及预后数据。
共识别出548例弥漫性世界卫生组织二级胶质瘤患者:2005 - 2008年诊断出142例,2009 - 2012年诊断出244例,2013 - 2015年诊断出162例。2005 - 2008年,64.3%的患者接受了切除手术而非活检;2009 - 2012年这一比例为74.2%;2013 - 2015年为74.1%(P = 0.08)。三个时间段的总生存率无差异(P = 0.11)。然而,对涵盖所有三个时间段的4个(共6个)中心的数据进行事后分析显示,2005 - 2008年的切除率为64.3%,2009 - 2012年为77.4%,2013 - 2015年为75.4%(P = 0.02),2009年及以后诊断的患者生存期更长(P = 0.04)。
在这项全国性的基于人群的研究中,我们观察到随着时间推移,LGG切除手术的比例呈上升趋势。此外,尽管由于可能存在混杂因素无法确定因果关系,但更积极的手术策略与更长的生存期之间存在正相关。