HIV-NAT, Thai Red Cross AIDS Research Centre, 104 Ratchadamri Road, Pathumwan, Bangkok, 10330, Thailand.
Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Rama 4 Road, Pathumwan, Bangkok, 10330, Thailand.
AIDS Res Ther. 2019 Apr 5;16(1):7. doi: 10.1186/s12981-019-0222-6.
Long-term success of cART is possible if the regimen is convenient and less-toxic. This study assessed the efficacy and safety of switching from a first-line NNRTI or boosted PI-based regimens to RPV-based regimens among virologically suppressed participants in resource-limited setting (RLS).
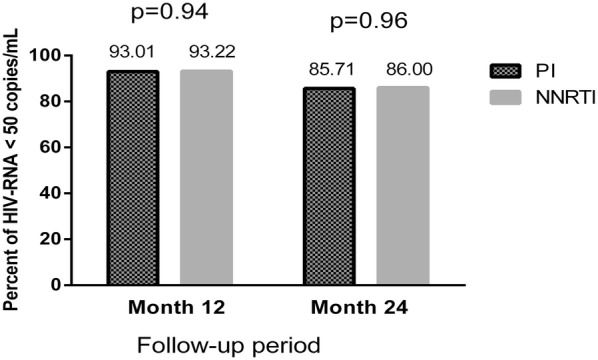
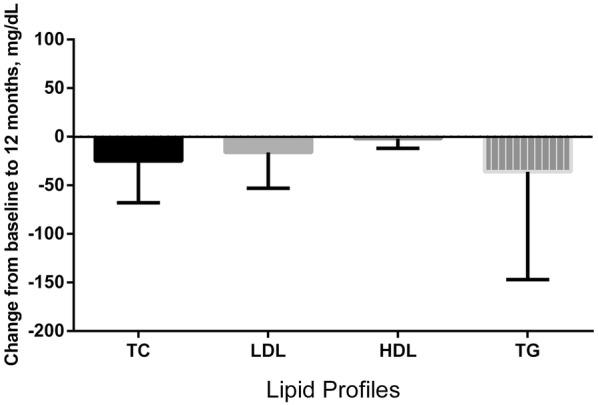
This is a prospective cohort study. Participants with plasma HIV-RNA < 50 copies/mL receiving cART were switched from a PI- or NNRTI-based, to a RPV-based regimen between January 2011 and April 2018. The primary endpoint was the proportion of patients with plasma HIV-1 RNA level < 50 copies/mL after 12 months of RPV. The secondary endpoint was the virological response at 24 months and safety endpoint (change in lipid profiles and kidney function from baseline to 12 months).
A total of 320 participants were enrolled into the study. The rationale for switching to RPV was based on toxicity of the current regimen (57%) or desire to simplify cART (41%). Totally, 177 (55%) and 143 (45%) participants were on NNRTI and boosted PI, respectively, prior to switching to RPV. After 12 months, 298 (93%) participants maintained virological suppression. There were significant improvements in the lipid parameters: TC (- 21 (IQR - 47 to 1) mg/dL; p < 0.001), LDL (- 14 (IQR - 37 to 11) mg/dL; p < 0.001) and TG (- 22 (IQR - 74 to 10) mg/dL; p < 0.001). Also, there was a small but statistically significant decrease in eGFR (- 4.3 (IQR - 12 to 1.1) mL/min per 1.73m2; p < 0.001).
In RLS where integrase inhibitors are not affordable, RPV-based regimens are a good alternative option for PLHIV who cannot tolerate first-line NNRTI or boosted PI regimen, without prior NNRTI/PI resistance. Trial registration HIV-NAT 006 cohort, clinical trial number: NCT00411983.
如果治疗方案方便且毒性较小,则长期使用 cART 是可能成功的。本研究评估了在资源有限环境(RLS)中病毒学抑制的参与者中,从一线 NNRTI 或强化 PI 为基础的方案转换为 RPV 为基础的方案的疗效和安全性。
这是一项前瞻性队列研究。自 2011 年 1 月至 2018 年 4 月,接受 cART 的 HIV-RNA<50 拷贝/mL 的参与者从 PI 或 NNRTI 为基础的方案转换为 RPV 为基础的方案。主要终点是接受 RPV 治疗 12 个月后,HIV-1 RNA 水平<50 拷贝/mL 的患者比例。次要终点是 24 个月时的病毒学应答和安全性终点(从基线到 12 个月时脂质谱和肾功能的变化)。
共有 320 名参与者入组本研究。转换为 RPV 的理由是当前方案的毒性(57%)或简化 cART 的愿望(41%)。在转换为 RPV 之前,总共 177(55%)和 143(45%)名参与者分别接受了 NNRTI 和强化 PI。治疗 12 个月后,298(93%)名参与者维持病毒学抑制。脂质参数有显著改善:TC(-21(IQR-47 至 1)mg/dL;p<0.001)、LDL(-14(IQR-37 至 11)mg/dL;p<0.001)和 TG(-22(IQR-74 至 10)mg/dL;p<0.001)。此外,eGFR 略有但统计学显著下降(-4.3(IQR-12 至 1.1)mL/min/1.73m2;p<0.001)。
在整合酶抑制剂负担不起的 RLS 中,对于不能耐受一线 NNRTI 或强化 PI 方案的 PLHIV,无先前 NNRTI/PI 耐药的情况下,RPV 为基础的方案是一个很好的替代选择。
试验注册 HIV-NAT 006 队列,临床试验编号:NCT00411983。