Stads Susanne, Kant K Merijn, de Jong Margriet F C, de Ruijter Wouter, Cobbaert Christa M, Betjes Michiel G H, Gommers Diederik, Oudemans-van Straaten Heleen M
Department of Intensive Care, Erasmus Medical Centre, Rotterdam, Netherlands.
Department of Intensive Care, Ikazia Hospital, Rotterdam, Netherlands.
BMC Nephrol. 2019 Apr 15;20(1):129. doi: 10.1186/s12882-019-1327-9.
Prediction of successful discontinuation of continuous renal replacement therapy (CRRT) might reduce complications of over- and under-treatment. The aim of this study was to identify renal and non-renal predictors of short-term successful discontinuation of CRRT in patients in whom CRRT was stopped because renal recovery was expected and who were still in the Intensive Care Unit (ICU) at day 2 after stop CRRT.
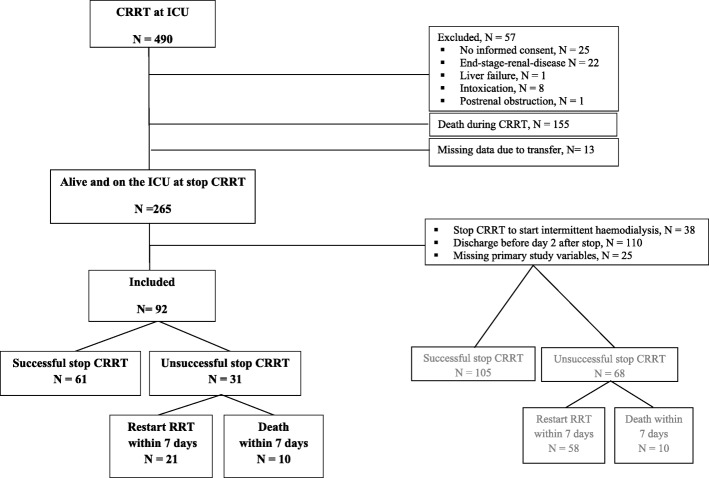
Prospective multicentre observational study in 92 patients alive after discontinuation of CRRT for acute kidney injury (AKI), still in the ICU and free from renal replacement therapy (RRT) at day 2 after discontinuation. Successful discontinuation was defined as alive and free from RRT at day 7 after stop CRRT. Urinary neutrophil gelatinase-associated lipocalin (NGAL) and clinical variables were collected. Logistic regression and Receiver Operator Characteristic (ROC) curve analysis were performed to determine the best predictive and discriminative variables.
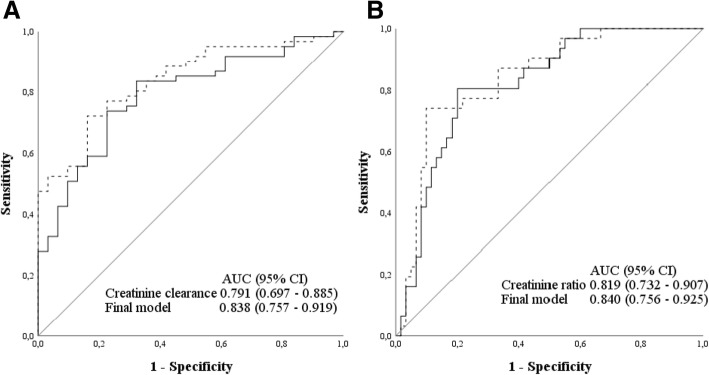
Discontinuation of CRRT was successful in 61/92 patients (66%). Patients with successful discontinuation of CRRT had higher day 2 urine output, better renal function indicated by higher creatinine clearance (6-h) or lower creatinine ratio (day 2/day 0), less often vasopressors, lower urinary NGAL, shorter duration of CRRT and lower cumulative fluid balance (day 0-2). In multivariate analysis renal function determined by creatinine clearance (Odds Ratio (OR) 1.066, 95% confidence interval (CI) 1.022-1.111, p = 0.003) or by creatinine ratio (day 2/day 0) (OR 0.149, 95% CI 0.037-0.583, p = 0.006) and non-renal sequential organ failure assessment (SOFA) score (OR 0.822, 95% CI 0.678-0.996, p = 0.045) were independently associated with successful discontinuation of CRRT. The area under the curve of creatinine clearance to predict successful discontinuation was 0.791, optimal cut-off of 11 ml/min (95% CI 6-16 ml/min) and of creatinine ratio 0.819 (95% CI 0.732-0.907) optimal cut-off of 1.41 (95% CI 1.27-1.59).
In this prospective multicentre study we found higher creatinine clearance or lower creatinine ratio as best predictors of short-term successful discontinuation of CRRT, with a creatinine ratio of 1.41 (95% CI 1.27-1.59) as optimal cut-off. This study provides a practical bedside tool for clinical decision making.
预测连续性肾脏替代治疗(CRRT)能否成功撤机可能会减少治疗过度和治疗不足的并发症。本研究的目的是确定在预期肾脏功能恢复且在停止CRRT后第2天仍在重症监护病房(ICU)的患者中,CRRT短期成功撤机的肾脏和非肾脏预测因素。
对92例因急性肾损伤(AKI)停止CRRT后仍存活、仍在ICU且在停止CRRT后第2天未接受肾脏替代治疗(RRT)的患者进行前瞻性多中心观察性研究。成功撤机定义为停止CRRT后第7天存活且未接受RRT。收集尿中性粒细胞明胶酶相关脂质运载蛋白(NGAL)和临床变量。进行逻辑回归和受试者工作特征(ROC)曲线分析以确定最佳预测和判别变量。
92例患者中有61例(66%)成功停止CRRT。成功停止CRRT的患者第2天尿量更高,肌酐清除率(6小时)更高或肌酐比值(第2天/第0天)更低表明肾功能更好,使用血管升压药的情况更少,尿NGAL更低,CRRT持续时间更短,累积液体平衡(第0 - 2天)更低。在多变量分析中,由肌酐清除率(比值比(OR)1.066,95%置信区间(CI)1.022 - 1.111,p = 0.003)或肌酐比值(第2天/第0天)(OR 0.149,95% CI 0.037 - 0.583,p = 0.006)确定的肾功能以及非肾脏序贯器官衰竭评估(SOFA)评分(OR 0.822,95% CI 0.678 - 0.996,p = 0.045)与成功停止CRRT独立相关。预测成功撤机的肌酐清除率曲线下面积为0.791,最佳截断值为11 ml/min(95% CI 6 - 16 ml/min),肌酐比值的最佳截断值为0.819(95% CI 0.732 - 0.907),最佳截断值为1.41(95% CI 1.27 - 1.59)。
在这项前瞻性多中心研究中我们发现,较高的肌酐清除率或较低的肌酐比值是CRRT短期成功撤机的最佳预测因素,肌酐比值为1.41(95% CI 1.27 - 1.59)为最佳截断值。本研究为临床决策提供了一种实用的床边工具。